
|
Psychoneuroimmunology (PNI) is a field of study that explores the interactions between psychological processes, the nervous system, and the immune system. The term is derived from three major components:
In essence, psychoneuroimmunology investigates how the mind and emotions influence the nervous and immune systems and how these interactions impact overall health. Researchers in this field examine the bidirectional communication between the brain and the immune system, studying how stress, emotions, and mental states can affect immune function and vice versa. The findings from psychoneuroimmunology research contribute to our understanding of how mental and emotional well-being can influence physical health and susceptibility to illness. It has implications for fields such as medicine, psychology, and immunology, providing insights into the complex connections between mind and body. What role do fascia and the interstitium play in psychoneuroimmunology? Fascia and the interstitium are connective tissue components in the body that have gained attention in various fields, including psychoneuroimmunology (PNI). While research is ongoing, here are some potential connections between fascia, the interstitium, and psychoneuroimmunology: Communication Pathways: Fascia and the interstitium are involved in communication within the body. They provide a network that allows signals to be transmitted between different tissues and organs. This communication system may play a role in the bidirectional communication observed in PNI, where psychological factors influence the immune and nervous systems. Inflammation and Immune Response: Both fascia and the interstitium are associated with the regulation of inflammation. In PNI, chronic stress or psychological factors can contribute to inflammation, and understanding how fascia and interstitial tissues are involved in immune responses may provide insights into the link between mental states and immune function. Neurotransmitter Release: Fascia contains sensory receptors, and the interstitium has been found to contain nerves. These structures may contribute to the release of neurotransmitters and other signaling molecules. The communication between the nervous system and the immune system, a key aspect of PNI, may involve these tissues. Tension and Stress Response: Fascia is involved in providing structural support and maintaining tension in the body. Chronic stress or psychological tension can affect the fascial system. Understanding how changes in fascial tension relate to stress responses and the subsequent impact on immune function is an area of interest in PNI. It's important to note that while these connections are being explored, understanding the precise roles of fascia and the interstitium in psychoneuroimmunology is still an evolving area of research. The interplay between psychological factors, the nervous system, the immune system, and connective tissues is complex and multifaceted. Finding metanalyses to cite this information directly is not available since this line of research is so new. The following are a few examples of where these conclusions/hypotheses are being drawn. Ball, T. M. (2011). Structural integration-based fascial release efficacy in systemic lupus erythematosus (SLE): Two case studies. Journal of Bodywork and Movement Therapies, 15(2), 217–225. https://doi.org/10.1016/j.jbmt.2010.10.006 Lupus is an autoimmune disorder. Though this article explores this one disorder, there are many other articles that explore the role of fascia and autoimmune processes. Bordoni B, Zanier E. Clinical and symptomatological reflections: the fascial system. J Multidiscip Healthc. 2014 Sep 18;7:401-11. doi: 10.2147/JMDH.S68308. PMID: 25258540; PMCID: PMC4173815. The Bordoni article talks about mechanical stress and inflammation’s role in interacting with the fascia system. I would argue that psychological stress is the same as mechanical stress because people generally tense and brace against stress. Bracing and tensing happen in the muscles and fascia, adding mechanical stress to the body. Poshattiwar RS, Acharya S, Shukla S, Kumar S. Neurological Manifestations of Connective Tissue Disorders. Cureus. 2023 Oct 16;15(10):e47108. doi: 10.7759/cureus.47108. PMID: 38022020; PMCID: PMC10646945. ^ This is an article that explores the connection between neurological and connective tissue functions, albeit by means of pathology. Gabor Mate, especially his book “When the Body Says No”, is a great resource for a more narrative exploration of PNI and the manifestations of “dis-ease” that result from stress. Exploring the connection between the fascia, psychology, neurological activity, and immunological processes provides an increasingly clear lever for healing trauma, its many challenging health manifestations, and a pathway forward to a sense of well-being in general, trauma or not. Ultimately, this budding research encourages us to keep moving, stretching, breathing, and developing our powers of attention and consciousness.
0 Comments
Here is an article by Robert Schelip on the way that fascia senses. He covers the five major nerve endings (Golgi, Ruffini, Pacini, the muscle spindles, and the interstitial free nerve endings) and how each can be stimulated to cause tissues to release.
He summarizes the takeaways at the end of the article:
Understanding how to relax and release fascia is important for not only healing from trauma but also for optimizing a sense of wellness and wellbeing. Think about a time you felt truly well. What did you feel in your body? People usually talk about feeling relaxed, strong, at ease, connected, and confident. Having a great deal of tension and lack alignment in your tissues can offset a feeling of ease and strength. When you approach trauma healing or even the pursuit of feeling your best, it is wise to consider your fascia because when your fascia is restricted or atrophied, you feel the sensation of that. it becomes a chicken or egg scenario. Are my emotions affecting my tissues or are my tissues affecting my emotions? It's important to take an inclusive view here. As we age we all approach a greater likelihood of chronic illness. Some of us start to experience the breakdown of the body much earlier than that. That does not mean we have to live with "dis-ease," however. For example, I have had chronic nerve pain off and on since age 16. Today I am a little over 6 months postpartum. It's no secret that pregnancy and birth is hard on your body. My nerve pain has been particularly loud lately, so I have my fascia on my mind more than usual these days. My pain comes from misalignment in my tissues. I use a variety of fascia strengthening and releasing techniques along with nervous system regulation exercises. Not only do I experience the realignment of my body as I rehab my system, I also experience waves of emotional release and nervous system discharge. I feel grateful for my education in bodymind regulation because, even though the regulation process can feel uncomfortable sometimes, I understand why I am feeling what I am feeling and can get to a calm, connected, and strong place quickly and reliably without having to cope or to deny my difficult feelings and sensations. Furthermore, fascia focused practices provide a surprising result. Even when I am out of alignment or in pain I still feel able to find that calm, connected, strong energy. I no longer feel that my sense of wellbeing hinges on being pain free or not having an emotion to process. I can stay connected to beauty and meaning no matter what I am experiencing in the moment. How interesting! As I learn to balance and regulate my bodymind, I feel less attachment to having everything sorted out inside. There is more of a sense of space and ease no matter what life throws at me, inside or out. I just found this essay I wrote back in June of 2022. As you explore the inner world of yourself and others, you will see there is a sort of underlying 'first principles' or rules from which our organization emerges. Give Them Some Oxygen 6/2/2022 Embracing the Hidden Wisdom Within: We all have parts that we don't like and try to smother. Parts that hold emotions that we reject, like anger, hate, weakness, sadness, shame, and wild pleasure. When we smother these parts, we dissect ourselves into arbitrary borders and dub some worthy and others unworthy. We become polarized and lose sight of what is wise about these othered parts. The Cost of Categorization: We do this because we feel those parts are costly. In our attempts to decrease our vulnerability, we become polarized in our thinking. We make some parts “good” and others “bad.” It is the categorization and labeling of these parts that is the origin of all functional mental illnesses. The parts that get smothered don't die, nor do they grow weaker, they instead struggle against their restraints and gag. They pop out sideways, acting out and demanding freedom to enact their wisdom. Reclaiming Wisdom: It's true that the unbridled expression of many of the parts that we reject, we learn to do because their expression was costly at some point. In our time of low understanding and lack of support, we make up stories about these parts so that they can never do the damage that they had done in the past. Ultimately, however, those urges that those parts have are wise in some way. They are pointing to something that we need either from others or from ourselves. As we mature and gain understanding and resources, someday, we can relieve the gag order and give these parts some oxygen. When we give these parts oxygen, it can be really scary. When those parts come, we feel the emotions that come with them. Perhaps there's hate, perhaps there is rage, perhaps there is a kind of blissful Mania that has no place in our home or business. When these parts come in, we feel those feelings we get scared that maybe we'll get stuck there, maybe the power I gained over this part will go away, and I will be overwhelmed by it. So, of course, in the beginning, it's important to do it with support, like Virgil holding Dante's hand in the Underworld. The Alchemy of Self-Discovery: We need someone who knows what they are witnessing to coach us through the intense sensation of the part as well as the intense reaction that we tend to have to that part. And with our hands held in this way, we are able to finally or at least start the process of seeing what this part is all about. And when we finally give this parts some oxygen, we begin to understand. Oh! We can hear the wisdom of what this part holds that we locked away when we locked away the dangerous aspects too. We get the opportunity to sort out that which is useful and that which is costly. In that sorting, this part has the opportunity to alchemize and transform into something updated that we can use now in our present lives. Trusting the Allies Within: We begin to see our parts as a gaggle of children in our charge. Never wanting to smother or deprive any of them but rather to lovingly understand and listen to the fate-altering, mind-blowing information that they have for us. And in so doing, finally, we get to reap the benefits of all parts of ourselves, updated and shown where we are now in our lives. We learned to trust these parts and give them access to the viewing room of our world. And when they see what we have become, they grow up to become whatever it is that we and they need them to be. We stop seeing these parts as enemies and instead see them as allies. We make amends for the misunderstanding and the defamation that we perpetrated on these sweet little beings.   I originally got this metaphor from my mentor, Steve Finn. Thanks, Steve!
Think of your emotional capacity like a bucket that can only hold so much. Everyone has different-sized buckets, and buckets can grow and shrink. When this emotional bucket overflows, it can lead to various reactions, from feeling depressed to getting anxious to getting angry. This post explores the importance of understanding these emotional limits, what happens if we ignore them, and the steps to help us recover. Inside the Emotional Capacity Bucket - Limits and Reactions: Everyone has a limit to how much stress they can handle and must find the right stress balance. Lack of “good” stress is also a form of “bad” stress, but that's for another article. Going beyond this limit can make some people feel sad, while others might get mad. In extreme cases, it might make someone think about making big changes in their life, like leaving their job, filing for divorce, or even suicide. Accumulating Stress: Once the emotional capacity bucket has been maxed out, every new stressor adds water to the emotional bucket, bringing you closer to “overflowing.” Even good stress pushes the person closer to the edge. People react differently to stress, so it's important to recognize that each person has their own limit. Expecting someone to behave or have the same capacity as you is misguided. Coping Requires Emotional Strength: Figuring out how to deal with problems requires emotional strength. If you’re already overwhelmed, it can be hard to express what you need or want. This is why typical “fix it” or “bootstrap (do-it-yourself)” interventions don’t work when someone is maxed out. Has anyone ever given you a lecture on mindfulness or told you to “take deep breaths” while you were overwhelmed? Or maybe they started giving you solutions saying, “Well, if you just did ‘xyz,’ you probably wouldn’t be feeling this way.” How did that feel? I personally believe coping should be used sparingly because it is much more efficient and effective to validate and allow difficult emotions to process through rather than trying to quell them with coping strategies. “Quelling” or soothing is really just gentle dismissing. Allowing emotions to process unburdens the person. The therapist or friend acts as a saucer who catches the overflow from the emotional capacity bucket. Listening and validating are the tools that help the excess water out of the bucket into the saucer of the person with more capacity in that moment. The beautiful thing about receiving the support of a good “saucer” is your bucket's capacity grows. Not only do you get relief in the moment, but you also are less likely to be overwhelmed by the same things in the future because you had the experience of surviving the hard situation and were supported enough to digest and reflect on what was hard about it. When you encounter something similar, your body and nervous system draw on the memory that you got through it before while in connection with a caring other. The embodied felt sense of that connection makes your emotional capacity bucket bigger, often even when no one is around. I want to note that in a world where good "saucers" and people with large buckets are limited, the vast majority are coping. I agree with Hafiz: “Fear is the cheapest room in the house. I would like to see you living In better conditions.” ― Hafiz Seeking Therapy Requires Emotional Strength: Telling an overwhelmed person to “just go to therapy” is harmful. Going to traditional psychotherapy requires some wiggle room in the stress bucket. If someone is already dealing with a lot, therapy might not be as helpful. It's a bit like trying to teach someone to swim when they've fallen off a boat—it might not be the right time. Getting bodywork that is focused on relaxation, neurofeedback, or supporting the person in carving out time for exercise, forest bathing, or alone time to do whatever they want can be much more helpful. Somatic Trauma and Attachment Therapists know how to work with the body without speaking and provide a viable alternative to traditional therapy for an overwhelmed person. See Emotional Injuries Like Physical Injuries When someone’s nervous system is maxed out and their bucket overflows, you must treat that person’s emotions like a broken bone or like the person who fell out of the boat in the earlier example. It is much harder for people to see emotional injury the way we see physical injury, but they are the same and often impact the nervous system similarly. Once you see it this way, you will feel silly if you find yourself arguing, dismissing, lecturing, or explaining to someone with an emotional injury. It will feel the same as arguing, dismissing, lecturing, or explaining to someone with a broken bone, like so: “Why are you crying? Everyone breaks bones. Don’t be such a drama queen.” “Why are you crying? Everyone gets anxious. Don’t be such a drama queen.” “Why can’t you help me with the groceries? It’s only a little broken.” “Why can’t you help me with the groceries? You’re just a little stressed right now.” “You know, I broke my arm once, and I was fine with it. It really made me a stronger person overall.” “You know, I had a panic attack once, and I was fine with it. It really made me a stronger person overall.” “Well, if you had paid more attention and not let things get out of hand, you wouldn’t have broken your bone. I’m not sure I want to take you to the ER. You need to learn your lesson.” “Well, if you had paid more attention and not let things get out of hand, you wouldn’t have become suicidal. I’m not sure I want to take you to the ER. You need to learn your lesson.” “Aw, come on, don’t complain about your broken bone. How do you think I feel?” “Aw, come on, don’t be angry. How do you think I feel?” “Oh wow! Your broken bone hurts so bad you've been in bed for days. Have you tried breathwork?” “Oh wow! You’re so depressed you've been in bed for days. Have you tried breathwork?” “You still have chronic pain? You’ve had that for 18 years! You should just get over it.” “You’re still sad about your childhood? You’ve been an adult for 18 years! You should get over it.” If you're the person with more emotional capacity, you may be thinking, “Well, it's not MY responsibility to coddle the emotionally injured person! What if I give in to their theatrics and make them weaker?” That is exactly the point I am making here. Validating and helping the person process the emotion makes them stronger. Dismissing and denying makes them weaker. You are actually making more of a problem for you and them down the road by trying to get rid of their problem rather than treating it like the injury that it is. It is the same as ignoring a broken bone. If I ignore a broken bone, it heals in such a way that the bone is weaker and more likely to break again. If I try to use the limb with the broken bone before it is healed enough, I reinjure the bone, and the recovery time is longer. Recognizing the Need to Stop: When something is wrong with our mental health, the first step is to recognize it and take a break to figure things out. Just stop. Then observe. That pause is so important. It can feel like swirly chaos, nauseating, clenched, imploding, exploding all at the same time. This is why people avoid stopping, but it is 100% necessary. Then observe. Take on a beginner's mind. Watch how you think, feel, and behave without trying to make any changes at all—just notice. Take the Pressure Off: Just like we wouldn't put weight on a broken leg, we should avoid things that add stress to our minds during the recovery time. Clear your schedule if possible. Taking medication might be a good idea. If you have to work, do the bare minimum. Take as many goals and deadlines off your plate as you can. Focus on the present moment for the most part. You may need to update your identity. The sooner you can take the pressure off, the sooner you will be able to reengage with life. The clients I have worked with who can stop quickly (and quickly is usually a six-month process!) have less to recover from because the pressure has not been piled on top of being totally maxed out for years or even decades. Clients who have been maxed out and who have had to “carry on” in that state with added pressure to “keep it together” take a lot longer to heal. I often have to sell stopping to people because social pressures to perform, achieve, and produce make people who stop feel shame. Choose the Right Professionals: Seeking help from professionals, like talking to a doctor for a broken bone, means working together to figure out what will help. It is important to find someone who understands the power of listening and validating. It does not matter how many degrees, how much clout, how many fancy techniques or medicines they wield. If your provider does not listen to you, they will waste your time and cause a lot more damage. If you feel ignored, dominated, or dismissed by your provider, leave immediately. This can be so, so, so hard when you’re already emotionally maxed out. You may not be able to do it, and that’s ok. Once you can muster the strength, start interviewing other providers. How you feel with a practitioner matters. Taking Small Steps to Recover: After taking a break, it's important to take small steps toward feeling better. This is like doing exercises to help a broken bone heal. You should move to this phase only once the bone is strong enough to do gentle physical therapy. On the other hand, not moving to this phase when it is time is also injurious. There are a lot of reasons people might avoid moving on to the active recovery phase:
Make Intentional Life Changes to Stay Healthy: Once the gentle recovery process has begun and we start to feel better, we can start to think about overall changes to make in our lives. Intentional changes that begin to emerge as a part of the healing process come with the belief: “Something wasn’t working, and I have agency to live a life that works for me.” Intentional change takes into account ongoing stressors like chronic illness, demands of your culture, needing to work, paying down debt, and other facts of life that might be present for you. Intentional change does not come from a place of ignorance or naivety. Rather, it takes stock and inventory of what is true now and what is possible from here. This differs from the changes made during a crisis. Changes made during a crisis often involve projecting all of the “bad” and blaming one person or situation or making broad sweeping generalizations about all of life itself (which can lead to suicide). Changes made during a crisis come with a belief that “if I just get rid of this one thing, it will ‘throw-away’ all the bad stuff in my life.” Understanding and respecting our emotional capacity is not only a personal responsibility but also a collective endeavor to develop a culture that truly understands and prioritizes mental well-being. Through awareness, validation, and intentional actions, individuals can navigate the complexities of their emotional worlds, promoting resilience and creating a foundation for lasting positive change. "The only way to make sense out of change is to plunge into it, move with it, and join the dance." - Alan Watts
Why do I keep getting into abusive relationships? Why do I stay in a job that I hate? Why do I keep choosing addiction when I know that I really want connection? I need to change, but I am scared and frozen. Why is that? Ancient Fear Human fear of change is a complex and multifaceted phenomenon rooted in evolutionary, psychological, and sociocultural factors. Avoiding change helped our early ancestors survive. They were much more subject to rapidly and dangerously changing conditions and needed to seek security to survive. Our ancestral instincts are incompatible with the conditions under which we now live. The result is that modern people stay “frozen” unnecessarily, or even to our detriment, in habit loops, unable to move on to a more enjoyable existence. The following reasons for fear of change come from our harsh beginnings and the nature of human social relationships that developed to meet our original challenges:
It's important to note that the degree to which someone fears change can vary widely, and some people are more adaptable and open to change than others. Furthermore, the context and nature of the change play significant roles in shaping individual reactions. Regardless of your circumstances, embracing change is a practice that improves when we bring intentionality to it. How do I increase my capacity to change? “Fear is a mile wide, and an inch deep. We perceive it as a massive ocean. Then we step into it, we realize it's just a puddle.” - Leila Hormozi Increasing one's capacity for change involves a combination of self-awareness, intentional effort, and a willingness to embrace new experiences. In many ways, embracing change is going against human instinct. You are not less of a person for feeling insecure while going through change. Rather, insecurity is to be expected because resistance to change is hardwired into us as a species. Here are some strategies to enhance your ability to navigate and embrace change while managing the inherent vulnerability and insecurity of the change process: Process Freeze States:
Change is a gradual process, and it's okay to take it one step at a time. Consistent effort, self-compassion, and a willingness to learn can significantly increase your capacity for change. Sometimes, a sense of urgency and the desire to rush change is a way to avoid change. This can stem from a fear of the change process. The urgency is trying to skip over the painful parts of change outlined in the first list above. Change can feel like jumping off cliffs. You can develop your relationship with the change process by jumping off curbs instead of cliffs to start to get used to the feeling of “falling.” Facing your fears does not mean you must be frozen in terror or bowled over by overwhelming emotions. If you look at change with an experimental attitude, you can take the pressure off of being perfect. Experimentation invites and expects mistakes. It values mistakes and failures as the fastest way to arrive at modes of living and functioning that work best for the given moment in time. Expect Complex Emotions and Be Ready by Knowing Your Own Complexity Have you ever heard clients (or loved ones, if you’re not a therapist and want to participate in the exercise) say things like this? What are the underlying emotional states you see in each example? (Suggested answers are at the bottom of the article.) 1. “I just feel so much rage, I literally see red. Like my vision is covered in a red film.” She said, visibly shaking in her seat. “If my colleagues knew, I don’t know, I could lose my job, or worse, my reputation. I’ve done things I’m not proud of.” 2. “I’m bad…” he stares off into space, “evil. There’s evil in me. I feel like I deserve all the bad things that happened to me. It's hopeless; I’ll never get better.” he pauses again, “I dont know if I want to get better. I want to die and take the whole world with me. Burn it all to the ground, you know?” 3. “When I think about what happened,” they said grimacing, “I dunno,.. Ugh!” they stuck their tongue out as if to vomit and lifted their hands, repulsed “It's just so disgusting, it's unbelievable! I CANNOT believe it.” 4. “I think I hate him…I HATE HIM!” he exclaimed, suddenly stopping in his tracks like a record scratch. His eyes stared off to a corner in the room, and all the life drained from his face. His voice faintly floated out of his throat, saying, “Oh wow, I was so worked up, but now I have no idea what we were talking about.” In the world of therapy, emotions are complex and varied, often bringing forth a rollercoaster of feelings for clients. As a therapist, it's crucial to expect and embrace the full spectrum of emotions that clients may experience during sessions. Here, I will explore the importance of acknowledging and creating space for feelings such as shame, anger, sadness, vulnerability, confusion, disgust, and even suicidal ideation. We'll discuss why attempting to "fix," "soothe," or "dismiss" these emotions is counterproductive and explore the role of dissociation in emotional processing. Moreover, we'll discuss practical strategies for therapists to navigate intense feelings, incorporating somatics and parts work into the therapeutic process. Embracing a Range of Emotions: Clients seeking therapy may experience a wide array of emotions that are often considered uncomfortable or challenging. It's essential for therapists to anticipate and acknowledge feelings of shame, anger, sadness, vulnerability, confusion, disgust, and even thoughts of suicide. By expecting these emotions, therapists can create a safe and non-judgmental space for clients to explore and express themselves. As you practice, you will start to recognize the “aesthetic” of an emotional state. The aesthetic is a multifaceted experience of the person that includes thoughts, emotions, sensations, postures, movements, body tension and collapse patterns, images in the client's and therapist's minds, and more. Sometimes people refer to the aesthetic as the "energy" or "vibe." The ability to recognize the aesthetic enables you to determine what emotional state is present faster and to validate the client experience more fully. For example, I can reflect that a client is sad because they are tearful. If I have a more complex relationship with aesthetic and I am attuned to the overall aesthetic of "sadness" in this person, I can reflect a shift to sadness before the client is fully in it, which increases rapport and trust in that the client feels acutely tracked and also feels “felt.” Furthermore, not all clients cry when sad. Acknowledging sadness when the client's expression might be more subtle, or the person’s sadness is generally not recognized or honored, can increase the client's awareness of sadness and help the client feel safe to feel the sadness now and increasingly as time goes on. This goes for any emotion, especially socially “inappropriate” ones. Thus, we heal the consequences of death by a thousand paper cuts that shove emotions down underwater. Many people have not been explicitly told to “not feel that feeling” but have gleaned from their environment that it is not okay to feel certain feelings. This is primarily done through dismissing, fixing, and soothing. The result is like trying to hold a life raft underwater: 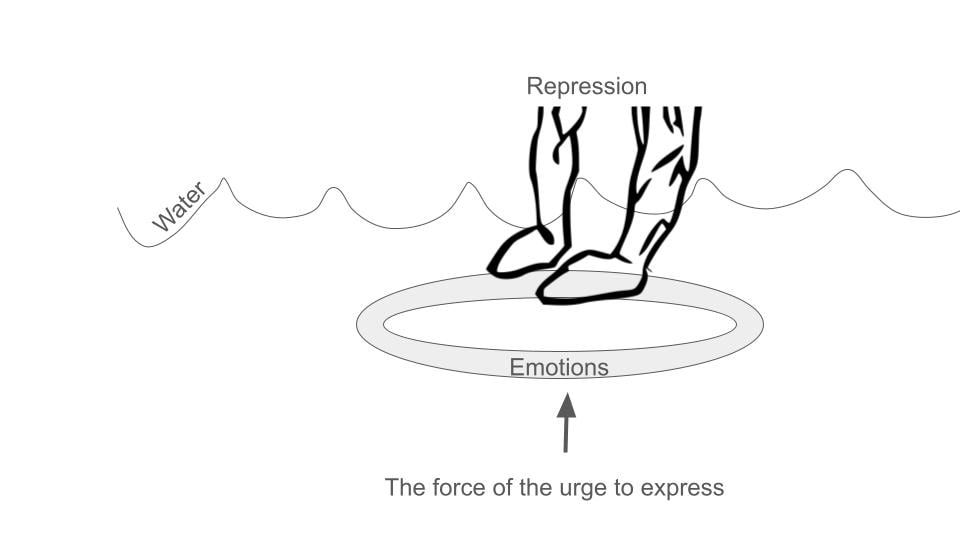 Avoiding the Urge to Fix or Dismiss: The impulsive reaction for many therapists, like those who trained the client not to feel in the first place, might be to alleviate their clients' discomfort by attempting to fix, soothe, or distract them from their emotions. However, these well-intentioned efforts can hinder the therapeutic process. Therapists should resist the urge to "fix" and focus on naming, validating, and feeling along with the emotions the client is experiencing. The exception to this rule is when a client dissociates; I will address that later. The reason that I see therapists have a hard time with this is that therapists have discomfort with their own socially unacceptable emotions. The only way for a therapist to get really good at validation is to be willing to feel fear, shame, disgust, and even suicidal ideation. The therapist needs to be unafraid to feel these feelings. Are you afraid to feel fear, sadness, loneliness, hopelessness, and the inner condition that causes suicidal ideation? If so, that means you don’t trust yourself to go into the emotional state and then come out of it. Another way to say this is that you don’t know how to regulate your nervous system at that level. Nervous system or emotional regulation does not mean that you are always serene and placid. It means that you can go into ANY feeling and efficiently find your way out. Ideally, what happens is the therapist feels a little bit of their version of the client's feeling, like rage, for example. Here’s how it goes down: The client looks tight; their jaw is clenched, biceps flexed, shoulder rounded forward, fists are starting to ball up, and their brow is furrowed as they talk about how, once again, their partner is making unreasonable, selfish demands. You say, “Wow! A lot of rage, huh?” Client: “Oh…my…god, I could punch a wall right now.” Therapist: “Oh yeah! Anyone would feel that way. I’m angry too hearing about this. Is it okay with you to feel this anger right now?” Client: “Yes, but I feel so stupid getting charged up like this.” Therapist: “Sure, that makes sense, you were taught it's not ok to be angry.” Client: “Right, anger was off limits. Mine was, anyway. What's the point of this anger anyway? It doesn't fix anything.” Therapist: “It's really uncomfortable to feel that much anger, huh?” Client: “Yeah, what do I do now?” Therapist:” What does your anger want you to know?” Client: “I am lonely and hurting.” Therapist: Oh yeah, can we just feel that loneliness and hurt together? Client: “Yes, that’s ok.” Therapist: “What’s it like to have someone feel this loneliness with you?” Client: “It's nice.” Therapist: “What's nice about it?” Client: “I do not feel alone; my anger can calm down. I feel like I can see my relationship in a different way.” This is an abbreviated example of validating, joining, and connecting the dots for the client and inviting the message of the feeling. There are many ways that this example does not capture how complex a dialogue like this can be, but the overall flow and format I present is something I experience repeatedly in sessions. Feelings are messengers. If we told the client to “try some deep breaths” when they wanted to punch the wall, we might not have arrived at the vulnerable feelings underneath. and we would not have been able to help the client feel connected. Notice how when the client feels connected and regulated, they can reframe their situation on their own. The therapist did not have to give them advice. This is the power of good implicit and explicit reflection statements, validation, and feeling with the client. It winds up being a lot less work for the therapist. Many therapists burn out, even in private practice, because they think they need to know everything or at least know a lot. Interpretive knowledge can help you steer the ship, but in actuality, you just need to know how to follow the client. That kind of knowledge is much less “expensive” than having to figure out how to interpret everything all the time. Understanding Dissociation: Many clients have learned that their feelings are not acceptable or valid, leading to dissociation as a coping mechanism. Therapists need to be vigilant for signs of dissociation, as it can be damaging if left unaddressed. Monitoring for dissociation and understanding its nuances is crucial for effective therapy. Rather than reacting to dissociation with panic or discomfort, therapists should strive to become competent and confident in handling it. Signs of possible dissociation include client reports and visible clues. Clients might report feeling confused, foggy, or suddenly feeling blocked while processing. Clients might not have words for what they are feeling, but you will get the hint they are dissociating because they suddenly look scared, frozen, or far away. Their speech may become slower, and more disorganized, their sentences might seem incomplete, or they may change subjects rapidly, becoming difficult to understand. It is important to know how to name the dissociation respectfully and artfully bring it to the client's attention. When a client dissociates, it means that something just “happened,” usually something that is “intolerable” for their system. Reassure the client that they always have consent and dont have to feel something they don’t want or aren't ready to feel. This reassurance can take the pressure off of the dissociation. I usually ask the client, “What was intolerable about what we were talking about just now?” Usually, the answer has something to do with “I’m not supposed to feel ______,” “I’ve trained myself not to feel_________,” “It’s too vulnerable to feel________,” etc. Rarely does a client recall a memory of which they weren't aware. Rather, it's usually an emotion or sensation that the client trained themselves not to feel long ago. Titrating Intensity with Somatics and Parts Work: To ensure the emotional intensity remains tolerable for clients, therapists can integrate somatic techniques and parts work into their practice. Somatics involves paying attention to the body's physical sensations, helping clients ground themselves in the present moment. Parts' work explores the various aspects of a client's personality or identity, facilitating a deeper understanding of their emotions without being consumed by them. The work, then, is to help the client learn to tolerate what has previously been intolerable. My aim with clients (and myself) is to be able to be present with any emotion or sensation. Once someone no longer has “off-limit” feelings, they experience much greater ease, clarity, and flexibility in life. It’s much easier to be continuously present. They can feel a feeling and efficiently find their way back to a healthy baseline, which is much easier to achieve if the therapist is constantly modeling regulation this way. It's a simple goal arrived at by a varied and nuanced path for every individual: Therapists play a vital role in helping clients navigate complex and challenging emotions. By expecting and embracing feelings of shame, anger, sadness, vulnerability, confusion, disgust, and suicidal ideation, therapists can create a supportive environment for clients to explore and express themselves. Avoiding the temptation to fix or dismiss these emotions, monitoring for dissociation, and incorporating somatics and parts work are essential strategies for therapists to foster a more profound and effective therapeutic journey for their clients.
Liz's Parts Work Journey
Studying non-dualistic spirituality in the tradition of Ramana Maharshi and my experience with clients during the first years in bodywork practice inspired me to see humans as multiple. Seeing humans as multiple contextualized a series of consciousness events I had growing up and in my early adult years. I am sharing this story because it highlights an underlying organization I feel in life. I believe that when someone discovers and interacts with this harmonious organization (aka spirituality, the "universe," the Game, the Tao, God, divine order and timing, etc.) in whatever way they name it, that the process of interacting with "it" is healing in and of itself. I discovered somatic parts work through a suggestion and a surprise. One day in 2010, my mentor, Steve Finn, told me, “Parts don’t go away, but we can throw them a retirement party or help them change their job description.” I adopted a “no parts left behind” policy from that day forward. At that time, I was also hyper-focused on non-dualistic spirituality from Ramana Maharshi's lineage and Eckhart Tolle's teachings. To see the good and the potential in others is a core tendency of mine, and this focus deepened my tendency to “see” the core essence of light and being in others. I have also been generally aware of the layers of disruption, anger, pain, and separation that layered on top of the core. The awareness of the layers increased at this time, too. I remember being confused as a young person because you couldn’t just interact with anyone and have an easy connection. I always felt like easy connection ‘should’ have been the case because I could “see” the core of perfection in others. Learning how the other “layers” or parts functioned helped me understand why the connection was so hard. Shift to Direct Communication with Parts As my clientele shifted to people with more significant trauma presentations, I began talking directly to parts. I would ask the parts and the client permission and invite the parts to speak freely. This was particularly easy with clients who had structural dissociation (the extreme version of this is called DID - dissociative identity disorder). It seemed to me that the parts needed someone willing to listen and go to the dark places with them. I was surprised that they tended to resolve on their own with good presence. I noticed that parts have their own postures and movement patterns, their own fascial restrictions, they hold disparate belief systems, and sometimes they even have their own mind/body dis-ease processes separate from other parts. Incorporation of Sensorimotor Psychotherapy (SP) My education in Sensorimotor Psychotherapy changed how I do parts work and added a new level of sophistication. I named my new Colorado-based therapy practice PROSOPON because I wanted to juxtapose the “prosopon” (πρόσωπον) or “parts that change,” i.e. masks or faces from the hypostasis (ὑπόστασις), “the essence that stays the same,” i.e. the non-dual core. This is one of the interpretations of this philosophical concept. (I also like how the “Os” in PROSOPON look like faces…to me anyway.) Philosophical Underpinnings and Education By the way, you see a lot of Greek and philosophy in my writing because I studied Latin for four years as a teenager and ancient Greek at my college, which is primarily a philosophy school (also called a great books program). I had the opportunity to study at the Zen Center in town concurrently. I am a great lover of evolving wisdom traditions and I bring them into my practice. Introduction to Internal Family Systems (IFS) I laughed out loud when I realized "how much time I wasted" (it's not really wasted time. The work was worth it and I wouldn't take it back for anything). I finally attended a 14-hour introductory course in Internal Family Systems this summer, the most recognizable version of parts work. I spent over 12 years developing my own approach when I could have just taken an IFS training. Fortunately, life is about the journey, not the destination. I took an introductory Janina Fischer training about her combination of IFS and SP (called TIST or Trauma-Informed Stabilization Treatment) this spring too. I must not have been ready to “get it.” I loved the training and incorporated what I learned, but it did not land like IFS. Accelerated Healing with Combined Approaches Incorporating the ideas of IFS, TIST, Sensorimotor, and my own style of approaching parts has accelerated the healing and recovery I have witnessed in my office. I am so excited to feel validated and educated by Dick Schwartz, his approach, and his community of therapists and trainers. The Implicit "Rulebook" for Parts Work The interesting thing for me is this: if I can develop my own version of parts work by interacting with client parts, as many therapists do, there must be an underlying implicit “rulebook” for how the human multiplicity of subpersonalities function. This reflects my experience with spirituality as well. When you simply turn your attention to something like the Tao, let’s say, over time, you start to get an embodied understanding of it that no word-based explanation can provide. The fundamental rule is that we are all multiple, and many of our mind-body and behavioral difficulties can be resolved if we start honoring, loving, and updating our subpersonalities as though they are real people. Key Modalities: IFS, Sensorimotor, and TIST I want to be really clear and transparent that I have yet to take level one of either IFS or TIST as of December 2023. I have taken introductory courses and studied material related to IFS and TIST, but I do not claim to practice these modalities per se. I incorporate my understanding of the philosophical and practical underpinnings of each modality. I love the IFS unburdening process because it's straightforward and user-friendly. Sensorimotor is magic surgery. SP properly applied manages a nervous system and its transformation better than any other modality I have ever witnessed. IFS helps SP get the job done by helping a client get to know their system, how to ask parts for genuine consent and learn about your non-dual core and how your parts relate to that core. The IFS framework creates an environment within which SP can do its magic. Importance of Regulation and "Titration" TIST highlights the importance of using parts for regulation and “titration” largely because Janina Fischer’s clientele, like mine, often have strong dissociation and overwhelm components. When an overwhelming feeling is present, we can't process it all at once. It's like being presented with a gigantic sandwich. I couldn’t eat the whole thing in one bite, but I can finish the sandwich if the bites are smaller and spread it out over multiple meals. When I recognize that an overwhelming feeling resides in just one part of me instead of all of me, it's like eating one bite of the sandwich rather than trying to choke the whole thing down. Pure Bottom-Up Somatic Work in Certain Cases There certainly are exceptions to this IFS and SP ordering. From time to time a client comes in, and they are so good at avoiding, or their nervous system is so disorganized that using emotional or sensing talk of any kind is unavailable. In these cases, I start with pure bottom-up somatic work, either myofascial release or somatic movement of some kind. Myofascial release is especially suited to help these clients because hardly any talking is required, and any talking that we do is related to purely physical things. Every time I have used this approach, the client begins to bring up emotional things on their own in their own time. You can read my article on trauma and fascia to understand more why starting with a pure MFR approach can be helpful for these presentations. I embrace the haphazard and, at times, comical nature of my journey (read “ignorance”), cherishing the continuous evolution of my 'selves' and therapeutic approach. The invitation to clients and clinicians is this: honor the journey, recognize the multiplicity within, and leverage the transformative power of somatic parts work. Trauma affects your fascia, but why should you care?
I care personally because addressing my fascia was key to my trauma-healing needs. I continue to regulate my nervous system with fascia care. I have seen the way my clients benefit. For some of my most complex cases, a course of hands-on fascia work allowed us to begin a healing process that sometimes ended decades-old symptoms. Clients have told me that the work can feel “psychedelic,” providing sudden insight, and “more relaxing than Xanax.” Those were just a couple of comments in the last few weeks. I could do a whole post on clients' reactions to the work (and I shall!). That seemingly simple body and touch work can produce effects as powerful as drugs without the hangover (usually) has completely altered my reality since I learned it in my mid-20s. It feels ordinary to me now, but I am constantly reminded of how amazing it is because my clients continue to react so strongly to it. “But why is fascia work so powerful?” you might ask. When I first encountered the power of fascia work, I asked this question, which kicked off a decade of voracious study on the topic. I will now attempt to give you a few distilled key points that can answer this question. The fascia and the nervous system occupy the same space in the body and are extremely intertwined. The fascia, a connective tissue, is intertwined with the nervous system as it contains sensory receptors called proprioceptors. These receptors provide information about body position and movement to the brain, contributing to the body's overall sense of spatial awareness. Additionally, fascia has been suggested to influence neural signaling and may play a role in conditions involving chronic pain or body system dysfunction (circulatory, digestive, lymphatic, immune, endocrine, etc.). Therefore, psychological trauma shows up in the fascial system. Psychological trauma can manifest in the fascial system through various mechanisms. Trauma may lead to increased muscle tension, affecting the fascia and potentially causing it to become tight or restricted. Chronic stress from trauma can contribute to the development of myofascial trigger points, which are hypersensitive areas in the muscles and fascia. Moreover, the body's response to trauma, particularly the fight-or-flight response, can create patterns of muscular tension and altered movement, impacting the fascial system. Emotional stress and trauma might also influence the autonomic nervous system, which can affect the fascia's tone and function. Research on the connection between psychological trauma and the fascial system is ongoing, and it's an evolving area of study within fields like psychoneuroimmunology and somatic psychology. Many of us in the Fascia and Somatic Fields regularly witness spontaneous memory recall when areas of an individual fascial system are released or when positions of past trauma (or even positions of neutral or pleasurable events) are experienced in a person's posture or body positioning. Fascial touch and movement techniques act on the Ruffini Endings and why that matters. Fascial release techniques, including stretching, “unwinding,” and a specific type of massage, may influence the fascia through various mechanisms, including stimulating Ruffini nerve endings. Ruffini endings are a type of proprioceptor found in the fascia that responds to sustained pressure and stretching. When myofascial release is applied, it can lead to a decrease in tissue tension and increased flexibility. The pressure and stretching stimulate Ruffini nerve endings, sending signals to the central nervous system that contribute to a relaxation response. This can result in a reduction of muscle tension and improved mobility in the fascial system. Since the fascial system is involved in all systems, including the nervous system, which is where psychological trauma is “stored,” trauma affects your fascia. Based on my personal, my colleagues, and my clients’ experiences, the current theory is that releasing fascia allows us to release some aspect of trauma stored in the central nervous system. Fascia also affects your trauma. The fascial system can put up to 2000 lbs per square inch on the body by means of restrictions that form in response to injuries and chronic psychological patterning. The brain registers this crushing force as danger and stress. When the circulatory, musculoskeletal, and other body systems no longer suffer the crushing pressure of fascial restrictions, they stop alerting the brain that they are in danger, thereby decreasing the overall stress load in the body. Big Caveat: much like mold illness, autoimmune disorders, and other stress disorders, while it is wise to treat restrictions at the body level (like treating mold symptoms through detoxification protocols), regulating your nervous system is ultimately more important. If you treat your restrictions without knowing how to regulate your nervous system, you'll be treating restrictions forever and wondering where is the benefit. Ideally, both happen at the same time. Why You Might Care. The profound interconnection between the fascial and nervous systems highlights the significance of addressing trauma through fascia care. The revelations stemming from personal experiences, as well as the transformative impact observed in clients, emphasize the potency of fascial work in trauma healing. The manifestation of psychological trauma within the fascial system, whether through increased muscle tension, the development of trigger points and chronic unexplained pain (think fibromyalgia and myofascial pain syndrome), or altered movement and posture patterns, emphasizes the intricate relationship between mind and body. The ongoing research in fields like psychoneuroimmunology and somatic psychology further validates the evolving understanding of how trauma “resides” within the fascia, so to speak. The tangible results witnessed by those in the Fascia and Somatic Fields, including spontaneous memory recall during fascial release, inspire hope in the potential of these techniques in unlocking and processing deeply embedded traumas. Fascial touch and movement techniques, by acting on the Ruffini nerve endings, offer a unique avenue for trauma release. The stimulation of these proprioceptors through pressure and stretching initiates a cascade of responses in the central nervous system, ultimately leading to a relaxation response. This process reduces tissue tension and enhances flexibility and mobility in the fascial system, which is intricately linked to all bodily systems. Thus, all body systems potentially experience renewed freedom in their function. In the process of trauma healing, the revelation that releasing fascia may facilitate the release of stored trauma in the central nervous system presents a compelling perspective. The comparison of fascial work to the powerful effects of drugs, without the undesirable side effects, speaks to the potential of this approach in promoting holistic well-being. As we continue to unravel the mysteries of the mind-body connection, the role of fascia in trauma becomes increasingly evident, providing new avenues for healing and resilience. 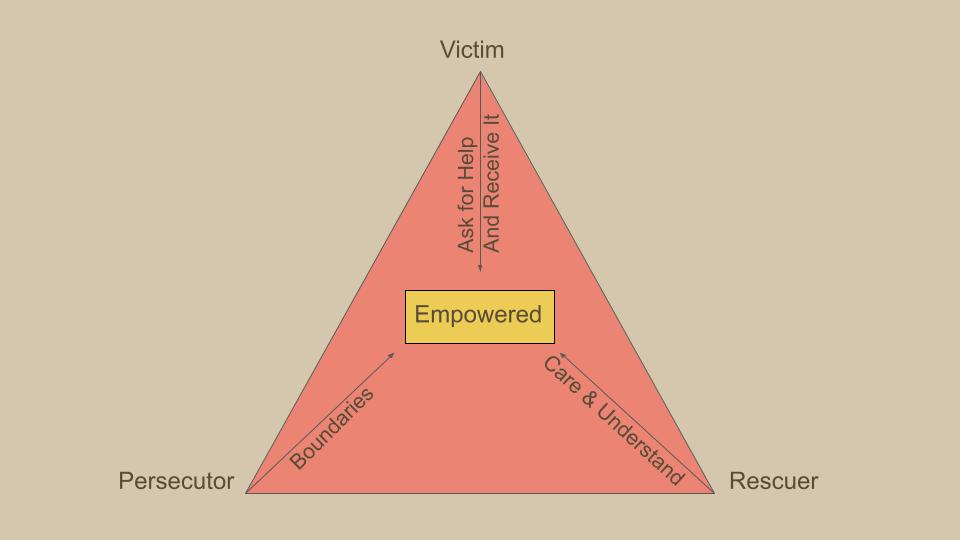 Karpman's Drama Triangle is a psychological model that explores the dynamics of interpersonal relationships and the roles people often unconsciously assume in conflict situations. Developed by Dr. Stephen Karpman, this model outlines three primary roles within the drama triangle: the Victim, the Persecutor, and the Rescuer.
This is a framework that clients often find helpful. Victim: The Victim in the drama triangle feels powerless, oppressed, or mistreated. They often portray themselves as helpless and may seek sympathy or external validation. Victims tend to avoid taking responsibility for their own circumstances and may inadvertently contribute to their feelings of powerlessness. Victims avoid personal growth by clinging to their victim status and blaming others.
Persecutor The Persecutor is the one who, consciously or unconsciously, takes on the role of the aggressor or antagonist. They criticize, blame, or attack others, creating an environment of conflict. Persecutors may feel justified in their actions and may not recognize the impact of their behavior on others. Persecutors avoid personal growth by devaluing and blaming others.
Rescuer The Rescuer is the individual who intervenes in the conflict, often with the intention of helping or saving the Victim. However, the Rescuer's actions can sometimes enable the Victim's sense of helplessness and may contribute to a cycle of dependency. Rescuers may also become frustrated if their efforts are not appreciated or if the Victim does not take steps towards self-empowerment. The Rescuer needs the Persecutor to persecute so that the rescuer can compare themselves to the persecutor and feel like a superior person. The Rescuer avoids personal growth by getting caught up in other people’s lives.
The Drama Triangle is dynamic, with individuals often moving between these roles in response to changing circumstances or triggers. What makes this model particularly insightful is its recognition that each role in the triangle can be disempowering and contribute to the perpetuation of interpersonal conflicts. Breaking free from the Drama Triangle involves individuals taking responsibility for their own roles and working towards more assertive, collaborative, and empowering communication styles. Doing so encourages self-awareness, accountability, and the development of more functional communication patterns. I am a fast processor, and I often attract fast-processing clients. People like us produce ideas rapidly. I also identify as a somatic person. I've spent a lot of time around people and groups that are intellectual and others that are somatic. Going through life as this combination creates dissonance. In somatic circles, I can be interpreted as disembodied. In intellectual circles, I can be interpreted as “out there.”
Internally, I feel congruent. When I observe misinterpretation, I notice it, feel a little disappointed, and reflect on how I truly feel inside. There is a temptation to get defensive. I want to explain myself. There is a misconception that you can’t be intellectual or a fast processor and simultaneously embodied. The truth is, you can presently embody whatever you are. You can even presently embody disembodiment. Speed has just as much a place in the body as slowness. Some bodyminds love speed. These body-minds often don’t do well with seated meditation and require other types of contemplative practice vessels. When you are choosing a contemplative style, choose one that feels good to you. White-knuckling through a 40-minute seated Zazen practice is not virtuous and misses the point unless your aim is to be present with limbic friction, which is also fine. Just be intentional that this is your aim. The point of a contemplative practice is to become present by repeatedly returning to a single focus. That could be a mantra or working on a Rubik's Cube. Your contemplative practice does not always need to be done as “time set aside” like a timed meditation. You could decide to return to your breath, sensations in your body, or something else, over and over while cooking or hiking in the woods. Doing focused timed practices is very helpful for learning presence and maintaining a strong connection to presence. If doing a timed practice is very irritating or brings up trauma, and that is not your aim, it's not time to have this as a part of your life. You may need some help from a therapist or spiritual person to work through your tangles inside. Once you have more inner clarity, you will love your practice in whatever form you connect with. Try a different practice if it feels like a chore or a battle. It might not be you. The practice vessel may be a bad fit. Types of Contemplative Practice Vessels:
What makes any of these practices contemplative is the quality of attention you bring to it. At first and in general, you practice keeping your attention on the thing you are doing. When your mind wanders, you bring it back. Over time, your relationship to contemplative practice evolves. You may feel an affinity for one specific practice vessel. Your preference may change to different practice vessels over time. It's important to know that it is not about any specific practice vessel (including seated meditation). The practice through any vessel is presence in the here and now. That is all. There is no aim other than this. The aim is not to “slow down,” “wake up,” “be better.” The aim is to be present and nothing more. “How can that be helpful?” You might ask. “Why would I want even to try this if it's not going to ‘help’ me?” Well, try it and see what happens. Let go of the mindful marketing out there that it's for this or that purpose, that you could become enlightened, or that you’ll be a better person. People have, understandably, used many tactics to convince others to do contemplative practices. They have used motivational and marketing hooks to get the job done. You may be reading this article because you want to be further convinced to practice. But why? Underneath all the teachings and mindfulness click-bait, there is something else entirely. I will not try to capture the “thing” or “not thing” in words. I can’t, and no one can. Lao Tzu famously points out the issue: The Tao that can be told is not the eternal Tao. The name that can be named is not the eternal name. The nameless is the beginning of heaven and earth. The named is the mother of ten thousand things. Try your hand at presence. Every time you do, invite total openness to what is. That is sensation, environment, inner experience, your life circumstances, the state of the world, that which you “know” and everything “you don't know,” and just see what happens next. If you're a fast processor or some other misunderstood type of person, don't try to “fix” yourself. There is nothing to fix. Be with who you are now and watch yourself become. Bodytherapy is Psychotherapy, and Psychotherapy is Bodytherapy.
There, I said it. This reality is a huge taboo, and its taboo status has been gnawing at me. My career and its current iteration are, of course, tied to my personal story. Confusion and fear were part of my foundation in life. I started seeking answers early. For example, I was obsessed with Maslow's hierarchy of needs when I was seven and when I was nine I declared that my family's ancestral trauma would end with me (still working on that one). I went through life on shaky ground. I could not do things the “normal” way. I always had many friends and achievements but felt like an outsider. I had my first real encounters with therapy as a teenager. I had a few psychotherapists in college. All the while, my condition declined. Finally, I met a psychologist and an osteopath, the first two professionals who treated me like a person. This is the foundation of good psychotherapy. Treating the client like they're a person. “If your other therapists weren't treating you like a person,” you might ask, “what were they treating you like?” At times, I felt that I was a paycheck, a diagnosis, a problem, a juvenile delinquent, an ego inflator, and a stupid teenager. I also kept waiting for someone to ask me, “And how does that feel in your body?” because I was feeling A LOT in my body. I was surprised they weren’t asking. My work with those two evolved into mentorship, shaping my modus operandi. One helped me understand transference/countertransference and parts work. The other introduced me to Osteopathic Manipulation and Katsugen Undo. Both taught me mindfulness and spirituality. I left the traditional career path and started a massage and yoga practice. Thanks to their help, I moved on from using medication and started working with a Functional Medicine doctor. Soon after, I was able to stop FM protocols, too. By then, I had completed yoga teacher training, learned Myofascial Release ala John F Barnes, learned energy work, and had done a TON of group therapy. I stopped using anything other than food, connection, and movement for my medicine. I felt free for the first time in my life. I seldom felt fatigued because every moment, I did things that made sense to me and regulated my nervous system. My clientele evolved. People who had gone through trauma and were living its psychological and physical consequences came for bodywork. Sometimes, clients would shift into sub-personalities, discharge their nervous systems, or spontaneously recall memories. When someone becomes a scared two-year-old on your table, you help them. You DO NOT tell them that this is not psychotherapy and that they need to “cut that out.” I did my best, but I knew I needed more training ASAP. I attended the Interpersonal Neurobiology Conference and learned about Sensorimotor Psychotherapy. One morning soon after, I woke up and wept. I knew what I had to do. I shut down my thriving practice in Austin and came to Boulder to learn somatics. I restarted my practice, got my degree, and got certified in Sensorimotor while in graduate school. I had the serendipitous opportunity to work with a Functional Neurological Disorders expert. My work with her brought all of my education together. Learning to treat FND was the final domino to fall, but I didn't know it then. I was too afraid to say it because I kept encountering this implied taboo. Here’s how it shows up:
I respect the needs of large mental health institutions and workplaces that train new clinicians. Graduate programs do have rigorous evaluation practices in some sense, but screening out clinicians who misuse touch (or power, for that matter) is a task that institutions can’t or are unwilling to do. I would have to do more research to really understand why touch is particularly taboo in graduate programs. Do we think new clinicians couldn’t discern that some clients would benefit and others would not? Do educators not want to take the time to learn about touch themselves? That touch is taboo in residential programs makes sense. I used to work at inpatient treatment centers for people living with psychosis. It was clear that the residents needed nurturing touch, but for that to occur between patients increased the risk of that touch turning into sexual contact and inappropriate boundary testing, something I saw many times. On the one hand, I think we ought to do our best to allow for platonic touch despite the risks, but I also understand why overworked, understaffed clinicians feel like they just don't want to deal with it. At a particularly high-end version of one of these facilities for people with psychotic disorders, clients were able to leave the campus to get massage therapy and PT, among other wonderful complimentary treatments. Psychosis with money looks vastly different from psychosis without, and touch is one of the things on which these clients spend their money. There are indeed whole sectors of the mental health field where integrating touch would be far more than a touchy subject. However, there are plenty of places where it is easy and makes sense, like private and group practices and some types of community mental health clinics with relatively high-functioning, resourced clients. I believe this bidirectional taboo persists out of habit, and it is time to redraw the boundaries. We may need a separate field or license for people who work with trauma from a nervous system perspective, or licensing boards could clearly state that specific integrations are appropriate for the license. Clinicians who work in an integrated way are not generally working outside of their license but are fearful due to a lack of clarity. For now, I will call the “field” Somatic Trauma and Attachment Therapists (STAT). STATs use:
STATs Treat
STATs support individuals' personal growth and evolution while acknowledging privilege/oppression dynamics and advocating for change in oppressive social systems. STATs receive education, training, and supervision from other STATs. This is a preliminary outline of the boundary of the practice of STATs as I know it and based on many hours of conversations I have had with fellow STATs. I am drawn to continue exploring what this field is as it stands right now and to document its evolution because it is certainly something that stands on its own with its own inertia moving in a direction. 11/27/2023 Video + Article: The Difference Between Sensorimotor Psychotherapy and Somatic ExperiencingRead NowAs the regional organizer for Sensorimotor Psychotherapy, I often get asked what is the difference between SP and SE. I did not create either of these resources but these are what I give to people who ask that question. I, unfortunately, do not have the name of the person who wrote the article but I do know that they were certified in both SE and SP.
Comparison Sensorimotor and Somatic Experiencing Somatic Experiencing and Sensorimotor Psychotherapy are two very distinct therapies with differing goals. Their founders had different objectives in mind; Peter Levine wanted to learn how to heal human trauma from observing animals in the wild, while Pat Ogden wanted to synthesize body and talk therapies to heal traumatic and developmental wounds. As a result, there are fundamental distinctions in their notion of therapeutic action; their understanding of the role of feelings, words, and thoughts in treatment; and their ideas about the therapy relationship. For example SP has developed specific techniques for emotional and cognitive processing, which plays a very important role in SP treatment. In comparison, because SE it is an approach based on animal behavior, it does not treat higher order functioning in the same systematic way that it treats autonomic nervous system imbalance for which it has a highly developed protocol. The distinction in goals and intention is clearly reflected in the overall structure and content of the training programs. While some of the techniques are similar because both incorporate a neurobiological model, they are elaborated in very different contexts. In SP the techniques are taught in relation to broad principles of practice, phases of treatment, and stages of the therapy process. Students are taught to apply SP techniques in accordance with certain criteria, i.e. whether the trauma is developmental or shock trauma, whether the phase of treatment is stabilization or memory processing. In SE on the other hand, the focus is not on the timing of the application of the technique but on the refinement and enhancement of the individual’s capacity to discharge arousal through such practices as titration, pendulation, resourcing and managing over-coupling between different elements of experience. After the first level of training, SP and SE completely diverge. The second level of SP deals with attachment patterns and character strategies and processing resulting emotions and limiting beliefs. In the second level there is an elaboration of the relational focus of the model with an emphasis on transference, countertransference and enactments. In contrast, the second level of SE applies the principal techniques of the first level to distinct kinds of categorical trauma like physical injury, horror, inescapable attack, emotional trauma and natural disasters. Training hours are spent on specific traumas within these categories such as drowning, electrocution, burns and car accidents. Which training should a practitioner choose? Pat Ogden’s broader project of combining talk and body therapies into a cohesive psychotherapy model to work with trauma and attachment is the mainstay of the SP training in the way that Peter Levine’s broader project of utilizing the technique of discharging excess arousal as a means of trauma resolution is the mainstay of the SE training. Which training a student would find more helpful is a matter of individual choice based on professional training and interest. Relationship: We believe that relationships that are respectful, empathic, playful, open, honest, curious, and properly boundaried are healing in and of themselves. We believe that the rupture and repair cycle is foundational to connectedness and, therefore, celebrate difference and conflict. The relationship is the foundation of our work together as clinician and client and among clinicians and partners in the practice.
Somatic Therapy: We use talk, touch, and movement that lead to greater awareness of the body, mind (nervous system), and spirit to create a secure attachment relationship with the body and minimize the noise of trauma. (Sensorimotor Psychotherapy, Somatic Movement, and MFR). Parts Work: We believe in connecting subpersonalities (prosopon - the parts of the human that change) to the core Self (hypostasis - the aspect of the human that stays the same), promoting a secure attachment relationship of the parts to the Self Spirituality: We believe that the realm of the spirit operates on specific rules/laws that one must discover for oneself. That discovery process is healing in and of itself. Interdisciplinary: We honor the contributions from other medical, therapeutic, healing, and cultural lenses. We celebrate working in a multidisciplinary/multicultural manner. Intersectional: We recognize the harm caused by institutionalized racism, ableism, homophobia, etc. We encourage clinicians, and partners to consider how we can reduce the damage of prejudice in our groups and institutions while also working to support individuals in improving their own lives despite ongoing oppression. Healthy Lifestyle: We honor that research science has proven that a consistent whole-food diet, strong relationships, good sleep hygiene, and regular physical activity can improve and modulate mood, prevent and treat physical disease, and foster a sense of well-being. We encourage clients and clinicians to adopt a healthy lifestyle in a manner suitable for the individual. We acknowledge limitations due to accessibility and work to shed light on systems that create barriers (e.g. food deserts, predatory marketing, and poverty). Harm Reduction: When addiction to a practice that is harmful to the health is present, we use a harm reduction model over abstinence. The reason for this is if the wound or underlying trauma that causes the harmful behavior is addressed, the harmful behavior will stop because the person no longer needs it. Contrarily, if abstinence is encouraged, clinician and client are liable to experience an unhelpful entanglement with each other and each other's parts, preventing the client from spending time where it matters most: working with the underlying wounds. Harm reduction can also be applied to people living with chronic illnesses of all kinds. Though there may not be an addiction present, we aim to reduce the impact of symptoms rather than attempting a complete “cure.” Pursuing perfection, in this instance, can be more harmful than helpful because the client can feel pressured to “be perfect” before reengaging meaningful activities. We believe that one can have a full and meaningful life while experiencing symptoms. I am not formally trained in IFS but I am trained in parts work. I find the IFS way of explaining parts work to be be especially helpful. So, you have a mystery illness…
Or cPTSD, dissociation, an autoimmune diagnosis, mold illness, MAST syndrome, POTS, etc. You've had symptoms for a long time. You have seen many doctors and specialists. Nobody has any answers for you. Now, you're in therapy because you are beginning to feel despair. You don't know what's going on. You feel some relief because you found a therapist who works with this situation, but part of you is already out of hope. Your back is against the wall. I am so familiar with this situation. In my early days as a bodyworker, many clients came to me in this condition. My own story has similar elements. Here is how I have seen this situation play out in therapy. Beginning Therapy First, we have to establish a connection between you and me. I am just another provider. You have no reason to trust me. You are probably feeling isolated, confused, misunderstood, and dismissed. My job, first and foremost, is to help you feel connected, understood, and validated. I wish I could help you with the confusion, but a lot of this is confusing to me, too. We will have to work together, possibly with other providers, to get to the bottom of this. People can find answers, and a lot of people do get better. When people don’t get better symptom-wise, they can often find a way to come to terms with their situation and live a fulfilling life anyway. Second, I support you in continuing to look for medical professionals, including functional medical practitioners, who can help you with your symptoms. It is not a foregone conclusion that you will need a medical professional, but you have symptoms, and it would be unethical for me to suggest that you should stop that search. Just because you have something that is hard for the medical field to recognize doesn't mean you don't have something that the medical field can help you with. Third, I begin to provide integrative somatic trauma therapy. That means I support you with somatic interventions and parts work. I encourage you to add movement and nutrition that works for you. We can add movement and nutrition professionals to your team if necessary and accessible. If you have a diagnosis that needs support from medical professionals, adding trauma and somatic therapy can only help. If you don't have a diagnosis and your symptoms are solely from your traumatized nervous system, then we will have already begun interventions that will help with your symptoms. Diagnostic Considerations When clients hear they may not have a diagnosis, they can feel dismissed, or they can feel relieved. If you feel dismissed, I want to assure you that just because someone doesn't have a diagnosis does not mean that what is happening isn’t real. What you are feeling is real; it may not be something that traditional medicine and therapy can help you with. You may have something that is not a classic medical diagnosis and would be better supported by a functional medicine doctor and modern somatic trauma therapy. If you need support from a functional medicine doctor, I will help you get that kind of treatment. I have supported many of my clients' engagement in functional medicine. The first time you begin functional medicine, it can be really confusing. It is often helpful to have somebody who has witnessed a lot of functional medicine cases help you navigate the immense amount of decisions that you're going to have to make on functional medicine route. Sometimes, clients start receiving functional medicine and ask me, “Do I really have to do all this? Can we just treat my nervous system and skip the medical aspect? Won’t my symptoms go away if I just have a balanced nervous system?” In my experience, the answer might be yes. However, the clients I have seen that heal the fastest follow some kind of health support along with somatic therapy. If you are symptomatic, that means your nervous system has been dysregulated for a long time, long before your symptoms emerged. Functional medicine, traditional medicine, nutrition, and movement interventions help alleviate and reverse some of the damage that has been done while we rewire your nervous system pathways. A multipronged integrative approach accelerates your healing. I will support you in making decisions about what protocols to follow and how much or little you want to do. Often, less is more (to a point). If you feel relieved that you may not have a diagnosis, that's great. The course of treatment on my end as your trauma therapist is the same whether you have a diagnosis or not. Whether you have a diagnosis or not, you will have experienced stress and maybe even a traumatized nervous system just from going through this mystery-illness-situation. If you do have a diagnosis, I will tailor what we are doing for that diagnosis. Furthermore, I will always tailor what we are doing to your unique situation, diagnosis or not. Phases of the Process People who come to me for treatment for a mystery illness, dissociation, or complex trauma tend to follow a similar trajectory that takes about two years. The following are the phases of the process. Slowing the chaos train takes about six months. This is where you and I are establishing rapport. I'm wrapping my head around the situation that you're in, and we are looking for ways to simplify your life without completely derailing you. I introduce you to parts work and we begin mapping your inner world. This period can feel like it gets worse before it gets better. Even though it feels like it's getting worse, I promise you it's starting to get better. Knowledge is power, self-knowledge even more so. “Mere” understanding can provide a lot of relief. Here is a caveat about the chaos train. Indeed, many can slow its roll in about six months but there are some exceptions. Sometimes a part of you is not done trying to do life "it's way." That's ok, it just means phase one takes longer. You know its over when you feel a clear feeling inside that says "I'm ready." Once you're ready, the rest tends to happen relatively quickly. You can still get a lot of preliminary work done before you're REALLY ready. Finding practices that genuinely work for you comprises the second six months. This is a period of experimentation and trial and error. We have an opportunity to learn even more about you and start to help give you more marked relief than the first six months. You'll get some relief in the first six months, but it starts to become more tangible in the second six months. Then, you deepen into your practices. In the third six months, we know a lot more about how you operate based on your responses to our trial and error experimentation of the second six months. This is when people start to really get a sense of relief. This is when you are in the “gym,” so to speak, applying the workout regimen that allows us to shift how your nervous system processes function profoundly. You can think of your former habits and processes like a well-cut trail in the woods. Your brain has been following a path that has been walked for decades. No plants grow on it. It is a deep rut of dirt. Now, we are creating a new path through the woods, one that works better for you. We are starting to pound out the dirt on this new trail, but it is thin and shallow and has a tendency to get overgrown. You begin to trust the process, and you begin to trust yourself in the fourth six months because you've started to see how these practices specifically tailored to you improve many areas of your life. If you have a diagnosis, it may not take away the disease or the disease process. Still, you do notice that it lightens your load physically and helps you have a more helpful belief system about your disease process that lightens your load mentally. You may even experience a decrease in your symptoms, something I've seen many times, too many to count. If you don't have a diagnosis and your symptoms truly are from trauma, it is common to see an almost total elimination of symptoms. At this point, you may not be symptom-free, but the difference between when you started and where you are now is so significant that you feel like you have performed a miracle. At this point, you have an orientation towards life and a set of practices that you can continue to do. Even if you are not symptom-free right now, you may experience the elimination of symptoms someday if you continue to practice cutting new trials in your neurological forest. Upsides and Downsides This process is not for the faint of heart. There are times when people regret having, as one of my clients puts it, “ left the shore” and wish they were back in the harbor. You may feel angry that you started this journey and scared that you left the tools that were “working” for you. You'll have to remember over and over again that those tools were also part of what brought you to therapy in the first place. This process is only for people who have a basic support system, unfortunately, because it is a destabilizing process. You also need a reason for why you are doing this process, whether that is more quality time with loved ones, a better quality of life for you, or the ability to express the gifts and talents you have that these symptoms cover up. Only you can decide if you are eligible to embark on this recovery journey. If you do choose to walk this path, whether you work with me or not, I commend you. If you choose to stay in the harbor, I respect your decision. This path is one of the hardest things anybody can do in life. This will not be like a typical accomplishment with public celebrations and awards. Some people will get it, and some people won’t. But if you undertake this massive task, you won't care what other people think because you will finally have the peace of mind and freedom that is yours and yours alone. Here is an essay by Dick Schwartz about the Larger Self. I love how he and his Internal Family Systems model conceive of what has been called "the higher self" and so many other names throughout history (Prana, Kundalini, the Atman, Christ Consciousness, Buddha Nature, neti neti neti (not this, not this, not this)). Since the earliest days of my work as a swim coach, I have emphasized orienting clients and students to their higher selves because to enjoy doing or achieving anything in this life truly, even the backstroke, we must first know our true nature. This essay of his discusses that Self.
Techniques that provide memory reconsolidation are a foundational element of the Prosopon approach. Ch 1 of Bruce Ecker's book Unlocking the Emotional Brain offers background information about these techniques.
Tracking the dynamics in the Polyvagal system help us know where you're at in your process so that we can use appropriate interventions that support your recovery and evolution.
No Time For Trauma
You’re in pain and have no time for this. Life is happening, and you’re sick of this crap hurting you and slowing you down, taking all your joy away. If you’re beginning trauma therapy, you probably want this to be over yesterday. By this, I mean your body symptoms, bad thoughts, anxiety, self-hatred, or whatever else you experience. I want that for you, too. That means you need to stop everything right now. The fastest way to address your trauma is to SLOW DOWN. That’s it. There is no quick fix or cutting corners. Everyone comes to trauma therapy like college kids to a get-rich-quick scheme. You may get some temporary results, but cutting corners will not create lasting wealth (healing). Not being traumatized anymore is a learned skill. There is no magic wand that will make you a champion skier, nor is there one that works for trauma. "I've tried to slow down, and I can't." Totally, I get it. I've been there. The first scary steps of the process take about six months on average. These first six months are all about decelerating the chaos train. It feels scary. Part of you thinks going fast is what you need. "I've lost so much time! I can't afford more time lost." Then hurry up and stop. Your current mode of operating got you this far, but it won’t get you where you need to go. Stop everything. Eliminate as much complexity from your life as possible but, more importantly, learn to stop your inner processes. This is sometimes called "thought-stopping." Stop explaining, understanding, worrying, scheming, searching, complaining,... Just stop everything and hear the silence within. Trauma is essentially a habit (called procedural learning). You don’t intend to do the habit. The habit happens when you’re not paying attention. That is why your symptoms seem to happen out of nowhere and why they seem out of proportion to situations you find yourself in. If you can stop, you can begin to track your trauma habits. Learning to stop is not the “answer.” It is the beginning of a long, strange trip to freedom. That Pain You Hide
“Many abused children cling to the hope that growing up will bring escape and freedom. But the personality formed in the environment of coercive control is not well adapted to adult life. The survivor is left with fundamental problems in basic trust, autonomy, and initiative. She approaches the task of early adulthood――establishing independence and intimacy――burdened by major impairments in self-care, in cognition and in memory, in identity, and in the capacity to form stable relationships. She is still a prisoner of her childhood; attempting to create a new life, she reencounters the trauma.” ― Judith Lewis Herman, Trauma and Recovery I like to write and think about Eudaimonia: The Good Life. Eudaimonia is a central value of mine that I pursue no matter the condition of my life: health, pain, joy, and sorrow. But I want to also address those who are going through the depths of trauma and stuckness. The way I write about Eudaimonia might give you the impression that I am not in touch with absolute intractable despair. I won't get your experience exactly, but my value of Eudaimonia comes from the experience of traumatization in myself and others. I will continue to write about what works and what health and healing look like because I believe that is more helpful than focusing on the pain (unless you're ready to "go into" the pain). But I also know that you need to know that I know pain before you'd be willing to hear about the medicine. I will try to demonstrate what I know about pain from time to time. Here's an attempt: To find yourself trapped in stuckness just as you've escaped the physical confines of the prison of your childhood (or some other suffering) brings a fear that paralyzes your very soul. It touches the indestructible essence of you, and, just for a moment, even the eternal, immovable part of yourself wonders why it chose life to begin with. What’s the point of this suffering? The suffering drags on and on—days spent sitting glazed, staring out the window, numb to the world. Or worse, you wriggle around with wretchedness, an inferno of panic burning up your insides as you wonder how much longer you can stand to feel this way. Perhaps you catch rage like how a smoldering coal erupts with fire with the slightest breath. Or you watch in disbelief while you compromise your values just to keep a little peace, while the moral fibers of your being scream at you, “No, not again!” but you are helpless against the fear of ruffling even one feather—seeing the slightest hint of discomfort or displeasure on the face of another. It goes on like this for years, maybe decades. You get by and find workarounds. Like a battered jalopy with mismatched doors and ill-fitting parts, you limp along the highway, white-knuckling it to your destinations each day. You come home both wired and exhausted (if you managed to leave your room at all), wanting nothing more than to sleep dreamless sleep, to feel what death might feel like, just for a moment, because you've determined that the end of life is the only way your chronic experience of chaotic innards will ever end. How is it possible I haven't just blinked out of existence? I feel I could vanish or explode or… But you don't sleep. You’re wide awake as the darkness of night taunts your pain “Relax! It's so serene!” as you feel a metallic grinding in the energy that pulses through every nerve in your body. The silence is like nails on a chalkboard, an endless drip of water on your forehead. It goes on like this for years, decades. “This is my life,” you think, “what a waste.” You hide your pain because when you don’t, you're told to “think happy thoughts” that “hurt people hurt people.” So you hide it all the best you can as you paint a mask on your face and modify your voice. Whole personas emerge to take care of daily tasks and keep food in your mouth (for what?). You are constantly isolated no matter how many sit with you at the table. Compliments, praise, and accolades mean nothing because your plastic facade is the recipient, and what feels like your “real” self is a bloody nub of a soul. Eventually, you can’t even keep that up. Your cardboard spaghetti western is soggy and collapsing. Everyone knows now… can't recover from this. So, you're at an impasse. “Do I kill myself or seek help?” Maybe you've already sought help, and it's all fallen flat. “Do I try again?” Part of you, way out at the margin of the map of your brain, has a shred of hope that something has to work. “It should work, shouldn’t it?” It's like a candle to an ocean, but somehow, that little pilot light of hope keeps you going—for years. It’s a miracle in and of itself. It's the miracle with which you start. Ground zero for a revolution led by your essence. No matter how bad it gets, a gentle, small voice whispers, “Keep going, you're almost there.” Out of options, you pray, “god damn, someone just show me the way already.” And in that moment of humble surrender, something inside quietly opens—something outside comes into relief: a person, a situation, an event, a book, a movie, a plastic bag blowing in the wind. The moment is marked with the ominous light of the morning sun during a solar eclipse. Everything looks the same, but something feels different. Suddenly, you're able to go to work. Not like your job, but a tiny start-up gem mine opens for business in your heart. You still struggle. You have a long way to go. Those old feelings linger and tug at you for a long time and still threaten to devour your bones, but something is different. That pilot light becomes a proper flame, and you can add larger, longer burning pieces of wood. As you huddle there alone at your little fire, someone joins you, and then someone else after that. You don't even notice that another body is curled next to you, adding warmth to your desperate scene. You and your company unwittingly band together against the elements. You understand each other, masks off. "Yeah, me too," you say, and the ice in your throats thaw into smooth chuckles of knowing. "What is this all about?" y'all ask as you look up to the starry ceiling, squinting your eyes and furrowing your brows as you try to penetrate the void with the will of an ant who does not know his size. Together, in your humility, the cosmic joke begins to dawn on you. Your suffering is the result of a thousand ancient accidents that humans have been trying to meditate and write their way out of since the dawn of civilization. You were set up to feel cursed with aloneness, but the punch line is that everyone is feeling that aloneness... together.
Retrieved from: europepmc.org/article/nbk/nbk493232#free-full-text
Anatomy, Fascia Bordoni B, Mahabadi N, Varacallo M Study Guide from StatPearls Publishing, Treasure Island (FL), 10 Apr 2018 PMID: 29630284 Abstract Researchers do not agree on one comprehensive "fascia" definition. Despite the scientific uncertainty, there is an agreement with medical text that the fascia covers every structure of the body, creating a structural continuity that gives form and function to every tissue and organ. The fascial tissue has a ubiquitous distribution in the body system; it is able to wrap, interpenetrate, support, and form the bloodstream, bone tissue, meningeal tissue, organs, and skeletal muscles. The fascia creates different interdependent layers with several depths, from the skin to the periosteum, forming a three-dimensional mechano-metabolic structure . The Fascia and Its Effect on Individual Health Three large groups of scholars have attempted to define fascia. The Federative Committee on Anatomical Terminology (FCAT), founded in 1989 from the General Assembly of the International Federation of Associations of Anatomists (IFAA), introduced the term "fascia superficialis" and "fascia profunda." The superficial fascia is a “whole loose layer of subcutaneous tissue lying superficial to the denser layer of fascia profunda.” The deep fascia, according to this definition, lies below the superficial fascia, highlighting two fasciae. In 2011, the Federative International Programme on Anatomical Terminologies (FIPAT), in agreement with FCAT, defined the fascia as “a sheath, a sheet, or any other dissectible aggregations of connective tissue that forms beneath the skin to attach, enclose, and separates muscles and other internal organs.” The FIPAT builds on the text of international anatomical terminology. The second definition specifies the term connective tissue, which functions to divide, separate, and support different structures. The connective tissue or fascia begins under the skin, excluding the epidermis from the fascia set. The third group of scholars is the Fascia Nomenclature Committee (2014), born from the Fascia Research Society founded in 2007. The board gave the following description of fascia: “The fascial system consists of the three-dimensional continuum of soft, collagen-containing, loose and dense fibrous connective tissues that permeate the body. It incorporates elements such as adipose tissue, adventitia, and neurovascular sheaths, aponeuroses, deep and superficial fasciae, epineurium, joint capsules, ligaments, membranes, meninges, myofascial expansions, periosteum, retinacula, septa, tendons, visceral fasciae, and all the intramuscular and intermuscular connective tissues including endo-/peri-/epimysium. The fascial system interpenetrates and surrounds all organs, muscles, bones and nerve fibers, endowing the body with a functional structure, and providing an environment that enables all body systems to operate in an integrated manner.” This is the broadest definition of fascia. The concept of a continuum of the collagen and connective structure, the cellular diversity that makes up the fascia, is emphasized. It is this continuum itself that assures the health of the body. These scientific definitions allow healthcare practitioners to make some deductions about fascia. The fascia includes everything that presumes the presence of collagen/connective tissue or from which it is derived. All the tissue considered as "specialized connective tissue" of mesodermal derivation is inserted into the fascial system. These include blood, bone, cartilage, adipose tissue, hematopoietic tissue, and lymphatic tissue. The fascial system has no discontinuity in its path, with layers of different characteristics and properties overlapping. A further research group for the nomenclature of the fascia founded in 2013: FORCE - Foundation of Osteopathic Research and Clinical Endorsement. The FORCE group has recently written several articles, highlighting new concepts to understand the concept of the fascia better: " The fascia is any tissue that contains features capable of responding to mechanical stimuli. The fascial continuum is the result of the evolution of the perfect synergy among different tissues, liquids, and solids, capable of supporting, dividing, penetrating, feeding, and connecting all the districts of the body: epidermis, dermis, fat, blood, lymph, blood and lymphatic vessels, tissue covering the nervous filaments (endoneurium, perineurium, epineurium), voluntary striated muscle fibers and the tissue covering and permeating it (epimysium, perimysium, endomysium), ligaments, tendons, aponeurosis, cartilage, bones, meninges, involuntary striated musculature and involuntary smooth muscle (all viscera derived from the mesoderm), visceral ligaments, epiploon (small and large), peritoneum, and tongue. The continuum constantly transmits and receives mechano-metabolic information that can influence the shape and function of the entire body." Anatomy, Fascia Bruno Bordoni; Navid Mahabadi; Matthew Varacallo. Author Information Last Update: July 17, 2023. Introduction Researchers do not agree on one comprehensive "fascia" definition. Despite the scientific uncertainty, there is an agreement with medical text that the fascia covers every structure of the body, creating a structural continuity that gives form and function to every tissue and organ. The fascial tissue has a ubiquitous distribution in the body system; it is able to wrap, interpenetrate, support, and form the bloodstream, bone tissue, meningeal tissue, organs, and skeletal muscles. The fascia creates different interdependent layers with several depths, from the skin to the periosteum, forming a three-dimensional mechano-metabolic structure [1]. The Fascia and Its Effect on Individual Health [2] [3] Three large groups of scholars have attempted to define fascia. The Federative Committee on Anatomical Terminology (FCAT), founded in 1989 from the General Assembly of the International Federation of Associations of Anatomists (IFAA), introduced the term "fascia superficialis" and "fascia profunda." The superficial fascia is a “whole loose layer of subcutaneous tissue lying superficial to the denser layer of fascia profunda.” The deep fascia, according to this definition, lies below the superficial fascia, highlighting two fasciae. In 2011, the Federative International Programme on Anatomical Terminologies (FIPAT), in agreement with FCAT, defined the fascia as “a sheath, a sheet, or any other dissectible aggregations of connective tissue that forms beneath the skin to attach, enclose, and separates muscles and other internal organs.” The FIPAT builds on the text of international anatomical terminology. The second definition specifies the term connective tissue, which functions to divide, separate, and support different structures. The connective tissue or fascia begins under the skin, excluding the epidermis from the fascia set. The third group of scholars is the Fascia Nomenclature Committee (2014), born from the Fascia Research Society founded in 2007. The board gave the following description of fascia: “The fascial system consists of the three-dimensional continuum of soft, collagen-containing, loose and dense fibrous connective tissues that permeate the body. It incorporates elements such as adipose tissue, adventitia, and neurovascular sheaths, aponeuroses, deep and superficial fasciae, epineurium, joint capsules, ligaments, membranes, meninges, myofascial expansions, periosteum, retinacula, septa, tendons, visceral fasciae, and all the intramuscular and intermuscular connective tissues including endo-/peri-/epimysium. The fascial system interpenetrates and surrounds all organs, muscles, bones and nerve fibers, endowing the body with a functional structure, and providing an environment that enables all body systems to operate in an integrated manner.” This is the broadest definition of fascia. The concept of a continuum of the collagen and connective structure, the cellular diversity that makes up the fascia, is emphasized. It is this continuum itself that assures the health of the body. These scientific definitions allow healthcare practitioners to make some deductions about fascia. The fascia includes everything that presumes the presence of collagen/connective tissue or from which it is derived. All the tissue considered as "specialized connective tissue" of mesodermal derivation is inserted into the fascial system. These include blood, bone, cartilage, adipose tissue, hematopoietic tissue, and lymphatic tissue. The fascial system has no discontinuity in its path, with layers of different characteristics and properties overlapping. A further research group for the nomenclature of the fascia founded in 2013: FORCE - Foundation of Osteopathic Research and Clinical Endorsement. The FORCE group has recently written several articles, highlighting new concepts to understand the concept of the fascia better: " The fascia is any tissue that contains features capable of responding to mechanical stimuli. The fascial continuum is the result of the evolution of the perfect synergy among different tissues, liquids, and solids, capable of supporting, dividing, penetrating, feeding, and connecting all the districts of the body: epidermis, dermis, fat, blood, lymph, blood and lymphatic vessels, tissue covering the nervous filaments (endoneurium, perineurium, epineurium), voluntary striated muscle fibers and the tissue covering and permeating it (epimysium, perimysium, endomysium), ligaments, tendons, aponeurosis, cartilage, bones, meninges, involuntary striated musculature and involuntary smooth muscle (all viscera derived from the mesoderm), visceral ligaments, epiploon (small and large), peritoneum, and tongue. The continuum constantly transmits and receives mechano-metabolic information that can influence the shape and function of the entire body."[4][5] Structure and Function Mechanical Function Normal movement of the body is allowed because of the presence of the fascial tissues and their inseparable interconnection, which allow the sliding of the muscular structure, the sliding of nerves and vessels between contractile fields and joints, and the ability of all organs to slide and move with each other as influenced by the position of the body. One of the fundamental characteristics of the fascia is the ability to adapt to mechanical stress, remodeling the cellular/tissue structure and mirroring the functional necessity of the environment where the tissue lays. For example, the plantar fascia in the foot adopts a mechanical model known as the "windlass mechanism" in order to provide dynamic support for the medial longitudinal arch while the limb transitions from the heel strike to toe-off phases of the gait cycle[6]. The fascial continuum allows the proper distribution of tension information produced by different tissues covered or supported by the fascia so that the entire body system can interact in real-time, including the epidermis. Emotional Function [7] The fascial unity influences not only movement but also emotions. Dysfunction of the fascial system that is perpetuated in everyday movements can cause an emotional alteration of the person. This emotional alteration could be established originating from constant myofascial nonphysiological afferents, which would bring the emotional state and the myofascial pathology to the same level. In fact, the position of the body stimulates areas of emotionality, and the presence of myofascial alterations leads to postural alterations. The myofascial system has a very fine, wide, diversified, and ever-present innervation. In particular, we can find the myelinated proprioceptive terminations (Ruffini, Golgi, and Pacini) inside or near the connective tissue in close relationship with the muscles where a multitude of very fine, unmyelinated-free terminations are in contact with the periosteum, the layers such as endomysium and perimysium, and in the connective tissue of all the viscera. These receptors are deputies to the functions of proprioception, nociception, and interoception. The afferent pathways of the interception project to the autonomic and medullary centers and to the brainstem, where they are sorted by the anterior cingulate cortex and the posterior dorsal insula, thanks to the thalamocortical extension. Interoception can modulate the exteroceptive representation of the body as well as pain tolerance; dysregulation of the pathways that manage or stimulate the interoception could cause a distortion of one's body image and influence emotionality. Embryology Many tissues derive from the connective tissue, such as blood, bones, cartilage, lymphoid and hematopoietic tissue, fat, tendons, ligaments, peri/epi/ endomysium, meningeal, all visceral communication, and coverage fasciae from the mesenchyme. During embryonic development, the connective tissue influences the form (morphogenesis) of the structures that it will contain and connect. The embryonic mesenchyme or connective embryonic or undifferentiated mesenchyme is formed by star-branched cells with a high mitotic rate (high reproductive capacity); they are considered pluripotent cells, as they can differentiate into different tissues. Embryonic mesenchyme will not only be the source of many connective structures but also stromal stem cells. During development, they occupy the spaces between embryonic layers by connecting the various structures and constituting the organ stroma. The mesenchyme is found and is derived from all three embryonic layers (ectoderm, mesoderm, endoderm), especially mesoderm and ectoderm. For current information and animal models, all structures within the fascia definition that form part of the head (muscles, bones, skin, etc.) and part of the cervical tract are derived from mesoderm and ectoderm. [8] Blood Supply and Lymphatics Blood and lymph derive from mesoderm and are considered connective tissues. In addition to the nutritive functions, blood also provides a way of linking to different organs which can communicate with each other through hormones and chemical mediators, guaranteeing the integration of the functions of the organism. The vehicle of immune cells and platelets can reach places where their presence is necessary; for example, areas of inflammation, of antibodies and proteins of the clotting system, and of the numerous transport proteins such as lipoproteins, transferrin, ceruloplasmin, and albumin to which the water-insoluble compounds that circulate in blood are attached. Blood is connective tissue. It consists of cells and cell fragments in suspension in an extracellular matrix of complex composition. The unusual characteristic of blood is that the extracellular matrix is a liquid, which means that blood is fluid connective tissue. There are two different components in blood that can be separated by centrifugation: (1) a fluid matrix called plasma and (2) corpuscles, which are cells or cell fragments. Corpuscles are erythrocytes, platelets, and leukocytes. Only leukocytes are complete cells; erythrocytes are anucleate cells, and platelets are cell fragments. Erythrocytes are present in larger quantities than the other elements, which is why they influence the value of the hematocrit much more than leukocytes or platelets, which make up around 1% of the total volume. Like the other elements, Erythrocytes are generated by pluripotent stem cells located in the bone marrow, particularly in ribs, sternum, pelvis, and vertebrae. There are different kinds of leukocytes. Granulocytes are characterized by the presence of big granules in the cytoplasm. They are visible in the optical microscope after coloring and are divided into neutrophils (with an affinity to neutral coloring), eosinophils (color with acid coloring), basophils (with an affinity to basic coloring). Lymphocytes, which include lymphocytes T, lymphocytes B, and natural killer cells, participate in specific defense: firstly, they recognize a pathogen, target it, and then attack it. The targeted answer implies almost always the production of proteins circulating in the blood, called antibodies. Monocytes are the biggest leukocytes, characterized by a big, horseshoe-shaped nucleus. The Lymphatic System The lymphatic system effectively removes the excess of interstitial fluids, solutes, and various cells and guides them towards the bloodstream, maintaining the volume of plasma and interstitial fluids in constant balance. The lymphatic system originates from the interstitial tissue called “initial lymphatics,” small capillaries delimited by discontinuous endothelium and basement membrane and low resistance to the flow of fluids and substances (hydrophiles molecules, cells, viruses, and bacteria). They attach to the external surface of the cells through collagen fibrils (collagen type VII). This collagen allows the transmission of mechanical forces towards the lumen of the lymphatic vessel; there is an autonomous contraction in some vessels, thanks to filaments similar to actin. These initial lymphatics become wider, creating collecting ducts that consist of collagen, smooth muscle cells, and elastic fibers. According to recent data, lymphatic vessels have their tone and, probably, their intrinsic contraction autonomy with a high ability of sensibility to flow variation (sensory functions). They are surrounded by nerves of the autonomous system, mainly sympathetic fibers, which could act to better coordinate the lymphatic transport. Lymphatic vessels adapt and change their elastic capacity, improving or worsening the function of lymphatic transport. There are primary valves formed by the cytoplasmic extent of the adjacent endothelial cells linked by close connections. The valves of these cells protrude towards the inside; this way, what goes in cannot go out. Finally, the intraluminal valves (weaker) are two sheets attached to the opposite sides of the lymphatic vessel and connected to zonules (perimeter junction involving a band that surrounds the cell). Lymph flows due to external mechanical compressions, for example, the one caused by muscle contraction and to its intrinsic contraction abilities. The lymphatic system is subject to aging, losing its elasticity and creating “aneurysms” over time, or decreasing the number of blood vessels or lymphangions (the lymphatic functional unit). Recent evidence reveals that lymphatic vessels are supported by a nervous system of vagal cholinergic type and sympathetic type, able to modulate the contraction (peristalsis, also helped by the breathing and pulsation of arteries) of vessels endowed with contractile fibers (with an actin-like protein). These thin nerves reach the external layer of the lymphatic vessel and then reach the deepest endothelial layer; this nerve network deteriorates in older people. The presence of both the parasympathetic and sympathetic systems is probably as tension or vessel tone modulators and as a sensor of the vessel's contractile layer. The Dural System The dural system has a lymphatic system called the glymphatic system. The cerebrospinal fluid (CSF) is drained through the venous system and the lymphatic system. Dural lymphatic vessels place themselves side by side to the veins and arteries of the brain; more specifically, they come out of the skull, following the reverse path of the pterygopalatine artery and a branch of the internal carotid, and travel through external vein paths to the skull and through cranial nerves that come out of the skull. Lymphatic vessels follow vein paths of the cribriform plate towards the nasal mucosa, following ways exiting the CSF. The lymphatic system absorbs the interstitial liquid and the CSF from the subarachnoid space and transports it outside of the skull, more specifically, from the base, up to the cervical spine. This mechanism is stronger during sleep. Nerves The innervation that affects the fascial system is autonomous: sympathetic and parasympathetic. The fascial system constitutes the same nerve structure (epi/peri/endoneurium). All layers are innervated and have a thin but potentially important plexus of nociceptors The sliding of the fascia structures that make up the nerve and the sliding of the nerve between the various tissues that it crosses and innervates is fundamental for the health of the nerve. Muscles Connective System Organization Gives the Shape of the Muscles [9] The fascial structure largely gives its ability to transmit the produced force. The latter not only functions as a transporter of the produced mechanical tension but stores mechanical energy to save myoelectric energy. The connective tissue that determines the various muscular layers derives in great proportion from the fibroblast. Muscles play a valuable role in managing the mechanical tension produced and felt by rapidly changing the morphology of their cytoskeleton; this mechanism is facilitated by the intervention of fibroblasts. If the mechanical stimulation felt by the myofascial system (connective and contractile tissue) is present for a short period, the morphological change will be transient. If the mechanical forces persist in reshaping the myofascial system, there will be a chronic change in form and function. Every fibroblast, potentially, is aware of the functional state of the one close to it as well as those distant from it, ensuring the fascial and mechanical continuity. In the connective tissue, there are other types of cells not yet wholly studied and cataloged. In the superficial and deep fascial tissue that covers and divides the muscle, cells like fibroblasts are called fasciacytes. These cells specialize in the production of hyaluronic acid (high molecular weight glycosaminoglycan polymer of ECM); the latter allows dampening of the tensions, fills the cell spaces, and allows sliding of the different tissue layers. They most likely will reside in the areas with the greatest presence of innervation (nerve endings, Pacini, and Ruffini corpuscles). Another type of cell found in the connective tissue is the telocyte. There are few studies on such cells in the fascial field, particularly for the latae fascia, thoracolumbar, crural, and plantar. They are found in many tissues of the human body and are involved in many biological processes. Telocytes form a network in the fascial network. They can form homocellular junctions (including telocytes) and heterocellular (telocytes and fibroblasts, endothelial cells, stem cells, adipocytes, etc.). Through these contacts, they can influence the metabolic environment and play a role in repair and remodeling. Probably, the telocytes can influence the production of hyaluronic acid. The exact role of these cells in the fascia is still unknown. Surgical Considerations Scars Surgical adhesions are the result of a lack of sliding between the various fascial layers. This absence or reduction of movement causes an inflammatory environment, which creates adhesions. The adhesions then vascularize and innervate, constituting an autonomous tissue compared to surrounding tissues. These adhesions could be the reason for recurrent pain in many postsurgical syndromes. Clinical Significance The muscular system is part of the fascial continuum, and in the presence of systemic diseases and disorders of the visceral, genetic, vascular, metabolic, and alimentary type, it undergoes a nonphysiological alteration of its function. The epigenetic processes lead to adaptation in response to a lack of mechanotransductive, causing a further decline in its properties.[10] Chronic Fatigue Chronic fatigue can be related to the fascial system, especially if the pathological disorder has been present for several years. If the fascia becomes fibrotic or if the layers of the tissues do not flow properly, bodily movements will be difficult. The movements will be uncoordinated, producing more anaerobic metabolites, which will be recorded by the central nervous system as fatigue. An example is fibromyalgia. Pain [11] [12] Increased levels of circulating cytokines from the connective tissue system, triggered by systemic diseases, could cause neuropathic pain. Connective tissue can directly send pain signals; it possesses nociceptors capable of translating a mechanical stimulus into painful information, and if there are non-physiological mechanical stimuli, proprioceptors can become nociceptors. The nociceptors themselves synthesize neuropeptides that can alter the surrounding tissue and form an inflammatory environment. The epineurium and perineurium are part of the fascial system innervated by nervi nervorum, which, if in contact with pro-inflammatory molecules, can cause sensations of pain and create a vicious circle. All the fascial layers need hyaluronic acid to slip one on the other. Decreased quantity or non-homogeneous distribution comprises the ability of local or systemic sliding of the connective tissue. There is much evidence that the change in the viscoelasticity of the fascial system is an important cause of nociceptor activation. Hyaluronic acid would become adhesive and less lubricating, altering the lines of forces within the different fascial layers. This mechanism could be one of the causes of joint stiffness and pain in the morning. An alteration of the adjustable tension may derive from the contractile capacity of fibroblasts, creating a fascial tone that is independent of neurological intervention. This contractile mechanism could cause an inflammatory environment with fibroblast hyperplasia, resulting in chronic inflammation and sensitization of nociceptors. The inflammation that can be registered by fibroblasts will increase extracellular edema that does not depend exclusively on the increased vascular permeability but also on the loose fascial tissue that recalls liquids inside it. The edema will bring an increase in tension and rigidity, with difficulty in sliding the fascia layers and the appearance of pain. The described framework will stimulate the fibroblast to release ATP (adenosine triphosphate), stimulating the nociceptors. The sensitization of nociceptors could derive from local ischemia caused by nonphysiological fascial tension, which prevents the proper functioning of the skeletal muscle and creates, for example, trigger points. Immune Response Fibroblasts influence the immune system and, consequently, the bone tissue; this relationship is osteoimmunology. The immune system and bone tissue share some molecular interactions, including transcription factors, signal molecules, and membrane receptors. In particular, osteoclasts sensitize cytokines and vice versa. When the fascial continuum fails to flow properly, its different layers, one on top of the other from the most superficial layer up to the periosteum, an inflammatory environment, acute or chronic, is created; the cytokines produced could stimulate the activation of osteoclasts and bone resorption, leading over time to an osteoporosis situation. Fibrosis or fibromatosis is the result of disorganization of connective tissue with hyperplasia and hypertrophy of fibroblasts due to a chronic inflammatory environment, nonphysiological mechanical stress, or immobility. It is a recognized calcification phenomenon. When fibromatosis is registered as similar to scar tissue, for example, in Dupuytren pathology, the percentage of fibroblasts that change into myofibroblasts increases, with alteration of the tension that the fascial continuum senses. This creates a vicious circle of inflammation and activation of nociceptors as connective tissue is much more sensitive to nociceptor activation than muscle tissue. Many chronic conditions, such as heart failure, chronic obstructive pulmonary disease, fibromyalgia, diabetes, always show alterations in the fascial system. These changes make the symptomatic picture more burdensome for the patient. Other Issues Researchers must always be impartial in the path of knowledge, because the results will be used by clinicians for patients. There should be no copyright on fascial terminology, because the researcher does not have to aim to make money. [13] References
Disclosure: Bruno Bordoni declares no relevant financial relationships with ineligible companies. Disclosure: Navid Mahabadi declares no relevant financial relationships with ineligible companies. Disclosure: Matthew Varacallo declares no relevant financial relationships with ineligible companies. Copyright © 2023, StatPearls Publishing LLC. This book is distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0) ( http://creativecommons.org/licenses/by-nc-nd/4.0/ ), which permits others to distribute the work, provided that the article is not altered or used commercially. You are not required to obtain permission to distribute this article, provided that you credit the author and journal. ID: NBK493232PMID: 29630284 Sculpting Marble
“The sculpture is already complete within the marble block before I start my work. It is already there, I just have to chisel away the superfluous material.” ― Michelangelo You can think of yourself beginning therapy as an unchiseled block of marble. Encapsulated in rigidity and chaos, you can't see your true form. In the right environment, the rough outline of who you are can come into relief in an instant. The first few sessions can feel immensely powerful because broad strokes are cut in raw material. It's exhilarating to see shape where before there was only rough rock. Then, the work begins. You start your work so willingly, and then the frightening corners of shame with their little monsters and cobwebs emerge on the edge of the light in the shadows. You pause. You balk like a spooked Mustang. And a really important thing happens. Your strategies and defenses show themselves; some clearly, and others with the guile of a holy coyote. The rough shape gets chipped and molded one brave trial at a time. Waves of dizzying heat roll through your body as you freeze before a dark corner. You stiffly point your toe to the edge, and the lip of darkness kisses the tip of your shoe. Your chest and face wash over with a burst of ice for an instant and then thaw into a sudden pool of calm as you pant and sigh out. It was only a child in there, in that darkness. You have been afraid of a child—a child who needs you. You pull her into the light and awkwardly sit by her side, your backs against the attic wall. She looks down at her feet as you inspect her out of the corner of your eye. “Am I enough for her?” you think to yourself. And then your heart melts, and your skin shivers as she quietly tilts her body, leaning her head on your arm, still looking longingly at her turned-in toes. “I’m so lonely,” she says as her bottom lip quivers and a single salty stream meanders down her cheek. You say nothing as you feel the small darkness of a soul grounded too soon. “I can handle this now,” you realize, “I can hold this child. I am more than enough.” Gradually, you gather your children, wraiths, and heroes together. You now see the hidden orchestra of your wounds, motivations, and workarounds. Approaching dark corners no longer causes fear. Perhaps you have some momentary anxiety from time to time, but you work through it quickly because you know that knowing is so much better than pretending that no one can see you because your eyes are closed. Your work has changed. Piece by piece, you polish your rough marble outline into an exquisite shine. And then, there you are, right here where you’ve always been, shining, reflecting the light back out so that you can be seen in your beauty, loved and admired. Now your work is brushing off settled dust, mending chips, and buffing scuffs. Occasionally, you add a little edit or a new fine detail or two, elaborating on the form that will always be you. Always in Training
The good life is a process, not a state of being. It is a direction, not a destination. - Carl Rogers I was practicing body work last week with a friend who also prefers the Eudaimonia (good life) path (See the post “Eudaimonia: The Aim of Therapy” to read more about the meaning of the word). He said to me, “We are always in training. The healing journey of the soul never ends. I won’t ever ‘arrive.’ This is so beautiful and so frustrating. I guess I have to figure out how to surrender to that.” I sat there and nodded, looking into the space in front of me. A slide show of memories paraded through my mind of the many moments I've been invited to surrender to the training-with-no-end. Many times I have also thought I would “arrive” and that I would finally do the thing that would allow me to fully relax and coast through the remainder of my days on this pale blue dot. At last, all I would have is peace and fun. Toil, fear, and shame would be banished from my being forever, and I would never have to deal with a difficult person ever again! I’ve also had to realize that no such end exists, that what I should be seeking is something entirely different, and that I needed to suss it out pronto if I am going to have my Eudaimonia. Oh! The grief I have felt letting go of that dream! Part of me chuckles that I mourn such waywardness. But hey, that other part of me who believes in the once-and-for-all really thinks she has “it:” the answer to all of life's problems. That is no small loss. What I am gaining now is not necessarily better than what I wanted life to be, but it is realistic and follows the rules of our reality here on this earth in these human bodies. So, in that sense, it is better. It's better because it works in this reality. It allows for what is instead of demanding what is not. I was trying to create an impossible fantasy. So what is it that I am gaining? A process and a direction. It's a shift from seeking a permanent state of contentment (control, gripping, getting high, walling-up, invulnerability, atrophy, fear, suspicion, distrust, hardness, shoulds) due to having gained the perfect material situation (money, beauty, fame, respect, being the best, etc.) to embracing the dynamism (allowing, letting go, groundedness, flexibility, vulnerability, resilience/anti-fragility, trust, love, suppleness, what is) that lets me know I’m alive. I now seek balanced aliveness. It's a special flavor of seeking that feels like constant calibration. I always want to seek the center (that is not to say I don't often fail, but I do try). Seeking: A Necessity and a Problem The drive to seek and progress is natural and innate. You can practice non-seeking, but even that is a kind of seeking. You are hardwired to seek. It's a fundamental part of being human. For any science nerds out there, Jaak Panksepp described the mesolimbic dopaminergic (ML DA) system responsible for all appetitive behavior and mental activity. You can’t get rid of it. It is so helpful and necessary, but it also causes so many problems. The ML DA is responsible for pursuing wants and needs, but it is also responsible for addiction. It is the foundation for our pervasive sense of restlessness and dissatisfaction. Seeking is central to our ability to survive. If, as a cave human, you gathered all the nuts and berries you need for today, sat down, and ate them all without getting more, tomorrow you would be hungry. If goals were deeply satisfying the way we want them to be, we would have never survived as a species. The problem is, now we have as many nuts and berries as we want, especially if you're in the majority of the developed world. If you are reading this, that is most likely you. While you are pursuing your goal, you feel good while you make progress. When you arrive at your goal, you feel rewarded and then immediately sad and depressed. Progressing towards a goal always feels better than completing a goal. This is why addiction is so compelling but feels so bad. With addiction, you artificially create an environment in your neurochemistry that makes you feel like you've arrived at the end of big goals over and over without having had to do the long-form work that big goals take. Another way to say this (for those of you who like neuroscience) is you are messing with the dopamine/serotonin/endorphin/oxytocin system. When you take the drug or do the behavior, you flood yourself with dopamine, which makes you feel like you're accomplishing something. Then you experience the effects of some or all of serotonin/endorphins/oxytocin, giving you a sense of completion, safety, connection, and/or a job well done. But it is artificial, so it does not hold up to the pressures of life. The addiction cycle becomes shorter and more frequent, eventually crowding out everything that actually holds water in your life. Completing a goal has a special feeling to it. It packs a big punch. But it is always followed by disappointment and sadness. This is why people make harder goals as they arrive at their original goal. You arrive at your goal and don’t feel the feeling you were expecting to feel, so you assume that there is something wrong with your goal and change the goal. But there is nothing wrong with the goal. The problem is your relationship to and understanding of what a goal actually is. Alan Watts has this to say about the “goal” of life: “We thought of life by analogy with a journey, a pilgrimage, which had a serious purpose at the end, and the thing was to get to that end, success or whatever it is, maybe heaven after you’re dead. But we missed the point the whole way along. It was a musical thing, and you were supposed to sing or to dance while the music was being played.” A goal is that at which you aim. Eudaimonia, a sense of well-being, comes from feeling progress toward a goal and also the spirit with which you walk towards it. Therefore, you need goals that you can never complete but are good to aim for. Goals like becoming wise, finding balance, understanding yourself and reality, and being honest in a tactful way. Then, you make these goals acts of play. You can never be done pursuing these goals because you can’t complete them. The music does not end until you draw your final breath. And then…who knows? It’s okay to have additional goals like making money, athletic achievements, career success, and traveling to new places. But since you can complete these goals, they should be small side quests or addendums to your endless goals. Side quests are best enjoyed in a state of play. Otherwise, you will persist as a being leading a life “of quiet desperation,” having it all except for a sense of satisfaction. I grew up around and have worked with many powerful people as a somatic bodyworker. There are people who are rich, famous, and fulfilled, and rich, famous, and broken. The difference has everything to do with the pursuit of endless goals versus the short-lived ones. On the other side of the coin, I have clocked many hours among the houseless and those of meager earnings. The same notion applies. I befriended a man of real fulfillment who lived in a tent on the cold side of the mountain in Santa Fe named Doc. He was beloved by whom he called the “residentially challenged,” as well as tourists, locals, and artists. I broke bread with my neighbor Herman, a former physics professor in Austin who took a vow of austerity in his later years. He had few possessions and prided himself on his ability to walk for hours around town. He provided personal aphorisms to me as little asides that moved mountainous earth in my young life, shaping the course I continue to take today. These two had little to show in terms of wealth or status (Doc was a little famous) at the end of their lives, but they were dripping with love and wisdom. Their abundance radiated from their beings and delighted those who could see it. People who are only focus on material goals miss the glory of these souls entirely because their being is not calibrated to behold the light of a full life well lived. That is not to say that Herman lived a better life than Bernie Madoff (the financier behind the largest Ponzi scheme in history). All things have their place in the world because the world “just is” it's not good or bad. But Herman was clearly fulfilled by his life though modest of means, and Bernie lost all he sought to attain because he built a faulty tower. He put all of the meaning in life into material things and died in prison with none of it. So, it's a matter of what choice you want to make. Do you want to build your life more on the stable ground of goals-with-no-end and playfulness, or do you want to tip the scales towards risking it all in the game of absolute materialism? Neither is wrong; it's a matter of preference and a spectrum at that. You can die in prison with nothing and still feel fulfilled as long as you had a few intangible goals in your your back pocket. You can be exceeding wealthy and famous and have Eudaimonia but it will not be due to the accumulation of wealth and fame. Lessons Along the Path The Eudaimonia path is always available whenever you want to walk it. In an instant, you can step onto it for the first time or rejoin your long relationship with it. The Eudaimonia path loves you and will never leave your side. That is why it is so easy to connect and reconnect to it, at least as far as Eudaimonia is concerned. And during the time before you join it or when you stray from it, it will consistently reach out to you, sending you little messages and beckoning you to return. The Noseo (ill-being) path wants you too, by the way, and has its own seductive nature. Your Eudaimonia will not be ruined if you choose to indulge in Noseo from time to time. In fact, a little Noseo enhances Eudaimonia. It's a matter of balance. So whether you are on the Eudaimonia path or are adjacent to it, as you seek and progress through life, you encounter the lessons of the path. These lessons are the reward of the Eudaimonia path. When you understand the lesson, you feel rewarded. Sometimes, when your connection to the path is not strong, you may not feel rewarded. You might feel shamed by the lesson like life is making fun of you or putting you in your place. Eventually, you feel that life loves you, is telling your stories, and teaching your soul. Or, maybe you don't understand the lesson. In that case, life loves you so much that it will increase the volume with which it teaches. In the words of a mentor of mine, “First life knocks on the door, then it kicks it open, then if that doesn't work, it will burn your house down, and it will continue to escalate until you understand the message and start loving yourself again.” This is the training protocol. The more competent you become walking the path, the more you will hear the knocks and avoid the escalations. The purpose of these life lessons is to get you focused on the “right” things. Now, before you take that as proselytizing, what I mean is the “right” things for you at that exact time in your life. Something that is right for one person is not right for the other. Something that is right for you right now is not right for you later. It is an extraordinarily subjective process. Practical Application of the Process Set Goals The process of Eudaimonia is an art form. You are looking for a balance between setting and pursuing goals while letting go of attaining the goals in a particular way. You also want to set attainable and relevant goals to your overall picture of well-being. An example of such a goal is running a mile without stopping as a new runner who eventually wants to run a marathon or learning to understand your parts (as in parts work) in the short term so that you can build a mature self in the long term. Dream as big as you can. This works for goals-without-end as well as side quest goals. Perhaps your dream is to become enlightened or to have a big, successful business. Let go of the outcome of ever attaining the goal, but work towards it anyway. Your big dream is the symbol of the path you are on. The point is not to get to the end of the path. The point is being on the path. Once you're on the path, you’re “there.” Being there is not enough, though; you must also progress along the path to feel a sense of satisfaction and delight. You will receive many gifts as you walk the path. Appreciate the gifts along the way, but never let go of your dream, no matter if you get there or not. Have a clear intention and light attachment. An intention is a guess where your efforts will take you. When you get information that conflicts with your intention, change your intention, but never let go of your big dream unless you want to change it to a different big dream. Make sure you have multiple big dreams so you don't get super fixated on one of them. If you start to get fixated, change focus. Prioritize Your Goals When you want to add new habits to your life that you aren't already doing, you have to put a special mental effort toward this change. If you want to run a mile and are not a runner, you don't have a part of you that craves running that will automatically remind you to get out there and train. Instead, running will easily get pushed down the to-do list if other tasks emerge during the day. So, you have to implement strategies to get yourself to prioritize practicing the new goal. Then, even if you successfully prioritize the new goal, you might find that when it is time to go on the run, you experience a lot of mental resistance. The resistance is normal and, unexpectedly, is the key to developing Eudaimonia, the good life. Eudaimonia is directly born out of the challenges and discomforts that you choose and prioritize in life. Noseo, ill-being, comes from the challenges and discomforts that happen to you. When I worked in the fitness world, I would say, “You can either feel sore from your workout or sore from having a weak back. You choose.” Take on Mini-Goals within Your Big Goals You want to avoid overwhelming yourself with your goals. Trying to do too big of a goal all at once will set you up to get discouraged and fail. If you have small enough goals, you will enjoy yourself. Completing these small goals will make you want to achieve the next small goal. You can have in your mind that you do want to run a marathon someday. It's okay to have lofty goals. You might plan to run a marathon next year and have a series of mini-goals that lead up to it. If you are consistent in your training but do not meet your mini goals despite your best efforts, it is better to change your goal schedule rather than try to force yourself to meet your arbitrary deadlines or to get rid of your goal altogether. Herein lies another aspect of the art and balance of the process of Eudaimonia. It is optional that you run the marathon or complete the lofty goal. It is important that you are consistently making that mental resistance in your system and choosing to practice consistently anyway. Even if you never run a marathon (maybe it's not right for your body for some reason), you have now developed a running habit that brings health to the body and mind (if running is the right form of movement for you). You do not have to be a fast runner or have incredible endurance to get these health benefits. Know When to Stop Working for the Day Quit while you're ahead, as they say. Keep a spark of spaciousness in your energy levels. You are playing the long game. Working really hard all at once because you are trying to get to the end of the big goal or mini goal as quickly as possible is the Noseo (ill-being) path. Paraphrasing Alan Watts: if the point of music were to get to the end, the best conductors would play the symphonies the fastest. We would go to concerts just to hear the big final notes, applaud, and walk out. Work done correctly is play. Children play until they want to rest, and then they do so, and so should we if our aim is Eudaimonia. Of course, your mileage may vary. Some people have constitutions that like to play hard for a really long time, and others only some. More is needed than a formula. You must know yourself. Set and Pursue Goals with Others If you are trying to do something particularly challenging for you or you want to maximize your work output, setting goals with others is the way to go. Trying to hold yourself accountable is lonely. Plus, you can turn your goal into a game. When you add other people, you create a sense of camaraderie; we’re all in it together. I don't want to let my buddy down. For some, a little competition is motivating. Crowd Out the Harmful with the Helpful Avoid things that erode your mental and physical health. This is often easier said than done, especially if you have trauma material to work through. Tasking yourself with eliminating bad habits completely is counterproductive. Harm reduction is often a better option. This is especially true of high relapse behaviors like addiction to substances, an eating disorder, and the like. If you've ever tried to kick a strong habit like addiction or an ED or know someone who has gone through this, you know that “Just Quit” is a silly directive. Rather, slowly working towards reducing the behavior over time, or at least performing the habit more safely, yields better results and allows the person to explore positive behaviors while still being able to do what has always worked for them. I've noticed that if you focus on adding positive things rather than taking away the negative things, the positive things begin to crowd out the negative things over time. If the person keeps adding positive things over time, sometimes the habit is completely eliminated. This can take years or even decades, but the elimination of the habit is more permanent than trying to quit cold turkey. To get your creative juices flowing, here is an incomplete list of things in no particular order to include and avoid if you want to build Eudaimonia: Include:
Avoid:
EUDAIMONIA: THE AIM OF THERAPY Every art and every inquiry, and similarly every action and pursuit, is thought to aim at some good; and for this reason, the good has rightly been declared to be that at which all things aim. - Aristotle Nicomachean Ethics Eudaimonia (εὐδαιμονία) is a Greek word that combines Eu, meaning well, good, easy, enriched, or abundant, and daimon, which refers to the complex Greek concept of supernatural power. Eudaimonia essentially translates as “good supernatural/holy/otherworldly spirit”. The word is also associated with well-being, human flourishing, and good life. Eudaimonia is the opposite of Noseo (νοσέω), meaning ill-being and mental and physical unwellness. It is no secret that humans (and all life forms) want the good and do not want the bad. Much of psychotherapy, coaching, personal training, physical therapy, self-help, etc., involves identifying your unique good and addressing what prevents you from having it. Psychotherapy, in particular, aims to help you develop the knowledge and organization of the Self so that you can live a life that is good for you and others. The following addresses these questions: What is the Self? What is Eudaimonia (healthy Self)? How do you build Eudaimonia? How does a therapist help you build Eudaimonia? I write this essay as an attempt to explain primarily to myself the nature of the goal of my work as a therapist and a client, as well as to describe the environment of the human psyche that I experience as “geometrical” for lack of a better word. What I mean by geometrical is that it is organized and has a visuospatial feel. My exploration is foundational, and I attempt to avoid going into too great of detail on anything because I want the underlying scaffolding of the psyche as I sense it to come into relief. I’ve used formatting and color-coding on key terms because I am describing diagrams (download the PDF above to experience the color-coding and formatting). I find that when I describe diagrams in paragraphs, the meaning can become murky without some visual aids for the reader. Before I continue, I want to acknowledge Dr. Paul Conti. As I began working on this piece, I happened upon his discussion with Andrew Huberman on the Structure and Function of Self and his definition of a “healthy self.” I felt inspired to expand on these concepts as I experience them. I also want to acknowledge Dick Swartz, Ph.D., founder of Internal Family Systems. I use some of his language when talking about the Self and parts. The work of these two people, along with many others, helps me put words to how I sense the structure of the human psyche in myself and my clients. The first part of this essay has a technical philosophical feel to it. If you do not like that kind of writing but want some practical thoughts on how to build Eudaimonia, skip ahead to the section called Healthy Character Structure (Eudaimonia) vs. an Unhealthy Character Structure (Noseo). What is the Whole Self? Color Coded Key of Terms (open the PDF link above to see color coding) Whole Self = “I am” Transcendent, capital-S Self = the higher self; feels like the “true” self to the Whole Self earthly, lowercase-s self = the ego/vehicle ridden/driven by the Whole Self to navigate the World of Form Structure of self = the organization of ego/vehicle Function of self = the action of the ego/vehicle Character Structure = the temperament and habits; type of vehicle and how it handles 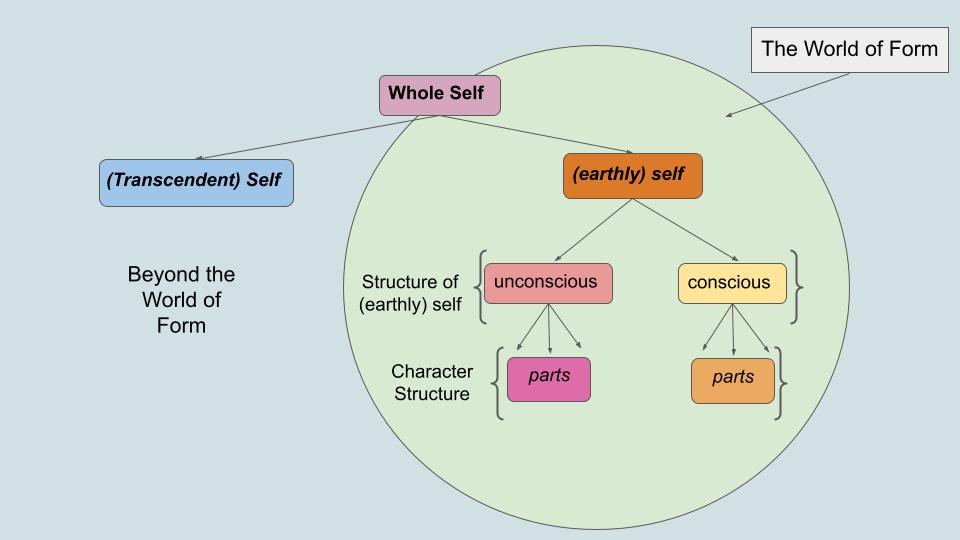 The Whole Self is what we mean when we say “I” or “me” (unless we have confused ourselves with one of our parts). It is made up of the transcendent, capital-S Self, which is indivisible, and the earthly, lowercase-s self, composed of the unconscious, the conscious, and parts. I’m using the words earthly and transcendent to get the gist of these aspects of self across. The World of Form in the image above refers to the earthly, material world we can see, touch, and interact with daily from birth until death. Beyond the World of Form refers to the realms of spirituality and other mathematical dimensions (think 5th through the 10th or however many physicists talk about these days), the great mystery. The (earthly) self has more to do with daily, egoic things. The (transcendent) Self is also involved in daily things but includes things outside of time and space. The (transcendent) Self experiences life but does not get damaged by, increased by, or caught up in life. The Structure of (earthly) self is how the (earthly) self is divided and organized. The Whole Self (Self+self) experiences all aspects of the self and does things out in the environment and inside the (earthly) self. This “doing” is called the Function of (earthly) self. The Function of (earthly) self is to engage in processes, behaviors, and defenses. The Whole Self is the “I,” as in “I am here; I am alive now.” The Structure of (earthly) self is the vehicle of the Whole Self. The Function of self is the action of the Whole Self; the driving of the vehicle. The Character Structure is how the Structure of self appears and acts. It is the type of vehicle you drive and how it handles. The Capital-S (transcendent) Self The “capital-S” Self is your sense of meaningful existence, your truest self, the real you. Different types of therapy view this self as a pure, higher self, free from wounding and unhelpful defenses. It is called the wise self, the mindful/resourced adult, the adult self, the larger self, the higher self, and so on. This (transcendent) Self feels calm and alive, connected to everything. I think of it as simultaneously interpenetrating and transcending the Structure of self, like a cloud that surrounds and fills the whole body and mind. It interacts with and “rides” the body and mind through this world. The (transcendent) Self both is the body/mind and is beyond the body/mind. When the (earthly) self harmonizes with the (transcendent) Self, you then have Eudaimonia: the good spirit. The Whole Self feels more like itself when it’s aligned with the(transcendent) Self. 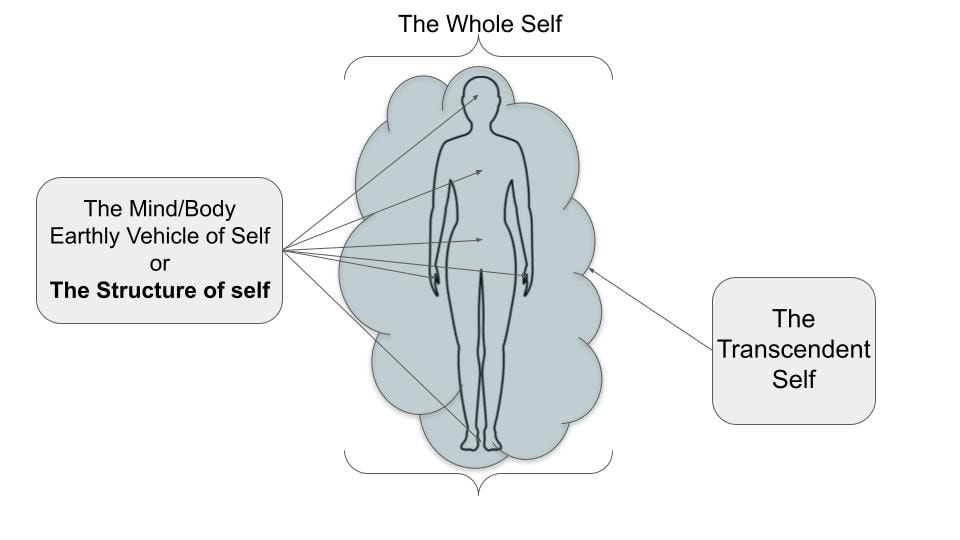 The Lowercase-s earthly self: The Vehicle The lowercase-s earthly self is often called the ego. We need it to interface with the World of Form. We often erroneously think we are the (earthly) ego self instead of the (transcendent) Self or the Whole Self, which is how the ego can become unhelpful. It’s like thinking that you are your car or bicycle and that your value is the same as your car’s value. Despite this challenge, the (earthly) ego self is necessary and useful. If we were only the (transcendent) Self, we would have no vehicle to move through the world. The Structure of (earthly) self The Whole Self is riding the Structure (vehicle). The Structure also anchors the (transcendent) Self to the World of Form. The Structure is composed of the unconscious and the conscious. The Structure can also be thought of as a collection of parts or sub-personalities. So, the capital-S Self is sort of like the primary or optimal personality with a transcendent quality to it, and the Whole Self is “riding” and using the parts to navigate the World (both the World of Form and Beyond the World of Form). The Whole Self is not the conscious, unconscious, or parts. The conscious, unconscious, and parts make up the vehicle that carries the Whole Self through the world. What is this vehicle made of? First, let’s talk about the conscious and unconscious. We’ll use Freud’s classic iceberg model to illustrate this: 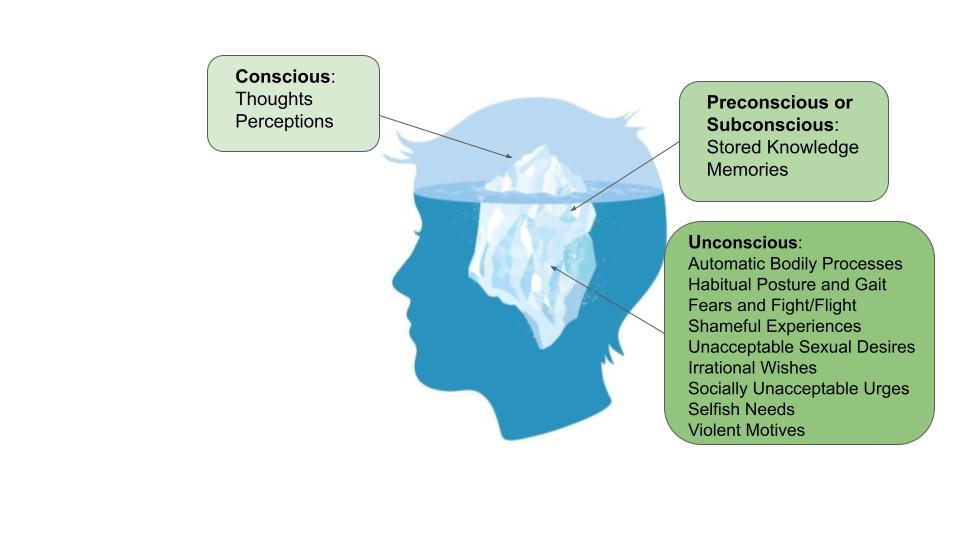 The conscious is the part of the mind we often (falsely) think of as the self. It thinks and perceives. We feel good when the conscious mind feels steady and in control. The conscious mind is vulnerable to confusion, fear, and despair. When the conscious is confused, fearful, or despairing, we do not feel good and can’t always make the best choices for ourselves or in our interactions with others. If we voluntarily go to therapy for the first time, that usually means that part of us can sense that the best choices are not being made by the conscious and/or we don’t feel good. Our safety is threatened if the conscious mind becomes extremely confused, fearful, or despairing. Think of someone with psychosis. They are often extremely confused, fearful, and despairing and can have a lot of difficulty navigating work, housing, and relationships. They often end up unhoused against their will. The preconscious or subconscious is the storage unit of the conscious mind. Nothing is super off-limits. These thoughts and memories might be useful later, just not right now. The unconscious is in charge of automatic things like your heart beating, lungs breathing, waste elimination, posture, gait, instinct to fight or flee danger, and seeking nourishment and safety. It also contains memories, thoughts, and feelings that are difficult and overwhelming for the conscious mind. The unconscious creates automatic defenses to protect the conscious from those things. The way the unconscious defends is part of the Character Structure. These defenses can be thought of as entire sub-personalities, aka parts. When the unconscious identifies a threat to the conscious mind, it sends thoughts and beliefs to the conscious mind and causes behaviors in the person to protect the conscious mind from getting overwhelmed. Parts and Character Structure Parts or Sub-personalities can be mapped onto Freud’s iceberg model. Parts reside in the conscious and unconscious and create the Character Structure. The Character Structure is your unique, individual appearance, flavor, and organization of your Structure of self. Anything other than the (transcendent) Self and the Whole Self is a part and, therefore, contributes to the flavor of the Character Structure. The Character Structure is the type of vehicle your (transcendent )Self and Whole Self are riding. 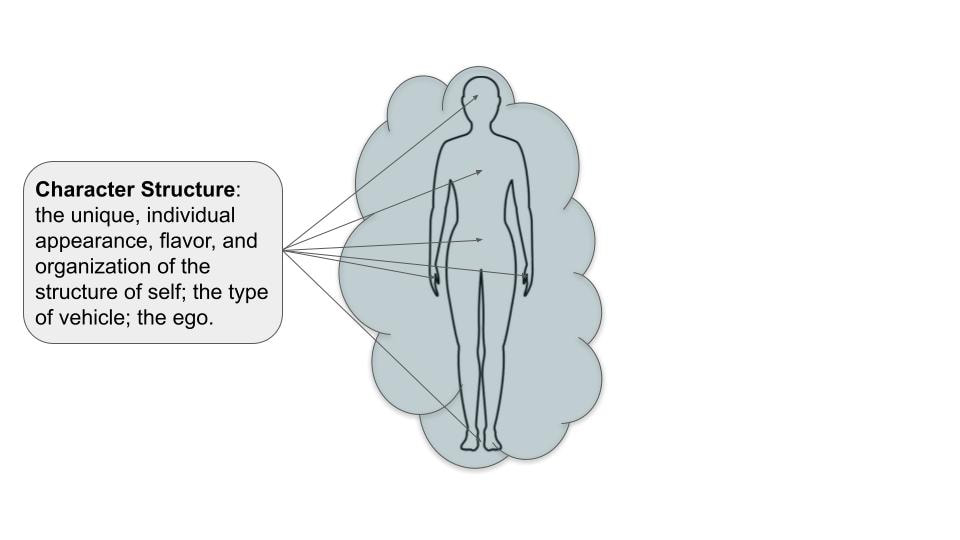 Here are a few examples of how parts are organized and function in the Character Structure: Part of me is altruistic, and part of me is jealous. Part of me likes to exercise, part of me likes to get cozy on a misty day, and so on. Each of these parts can be thought of as whole sub-personalities. The part that likes to be cozy has different emotions, motivations, values, and preferences than the exercise part. Both the exercise and the cozy part are considered acceptable. When I’m in my cozy part, my exercise part is in my preconscious, ready for use when the time is right. Parts that are not deemed appropriate or acceptable are hidden in the unconscious. Let’s take the jealous/altruistic parts to continue with the example. The jealous part is in the unconscious because jealousy is considered a shameful emotion in my culture, so I’m going to attempt to hide that from myself and others. Even though it’s hidden, it still exists and has a role in the system. Altruism is a valuable quality in my culture, so I am comfortable being conscious of this part. It’s not that altruism is always good or jealousy always bad. My learned cultural shame, however, hides the jealous part from me. Controlling misplaced jealousy is good, but denying it altogether is not good because that part will act without my knowledge. Protective parts that act on my behalf without my knowledge also reside in my unconscious. Like clandestine secret agents that protect countries behind the scenes, these parts have determined that the system shouldn't know their existence. If the system knew these protectors, it would compromise their mission. For example, let's say I have unconscious social anxiety and can quickly become overwhelmed socially, but at the same time, I want to see myself as socially resilient. My conscious thinks of me as socially resilient, and my unconscious thinks of me as quickly overwhelmed. To maintain my view of myself as resilient and not anxious, my unconscious will guide me, without me knowing it, to avoid situations that would reveal my anxiety to me, thereby protecting my consciousness from being overwhelmed. To further illustrate this, let’s say someone criticizes a public speaker, saying, “I could do a better job!” but never pursues public speaking. When asked why I don't pursue public speaking, I’ll say, “Oh, I’m just not interested,” when I actually unconsciously fear public speaking. I criticize the public speaker because the speaker symbolizes fears I have not faced but unconsciously wish I could. Criticizing the symbol is an unconscious attempt to devalue the achievement (getting in front of an audience and presenting) so I can continue avoiding the motivation to pursue that goal. The upside is that avoiding pursuing this goal prevents my conscious mind from being overwhelmed. The downside is I forgo both becoming resilient and doing something that I might enjoy. 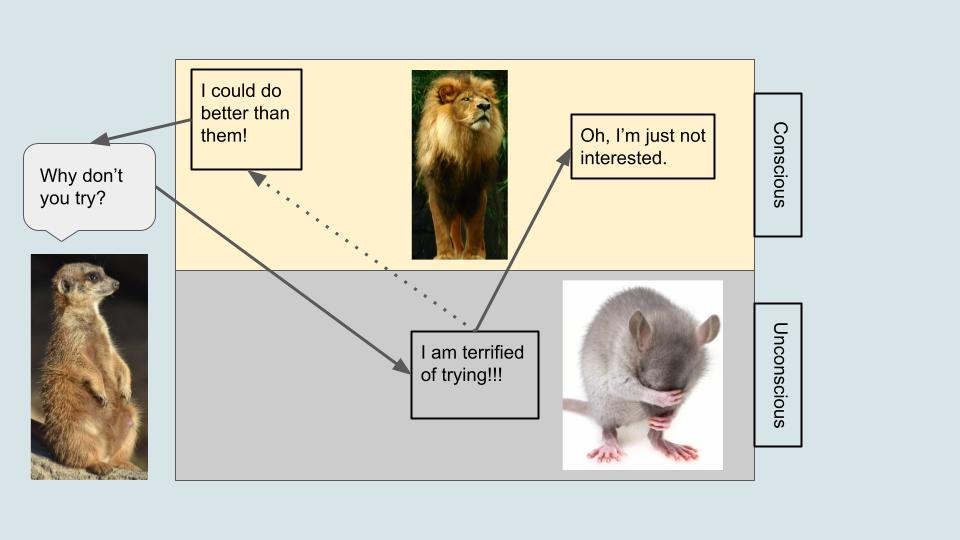 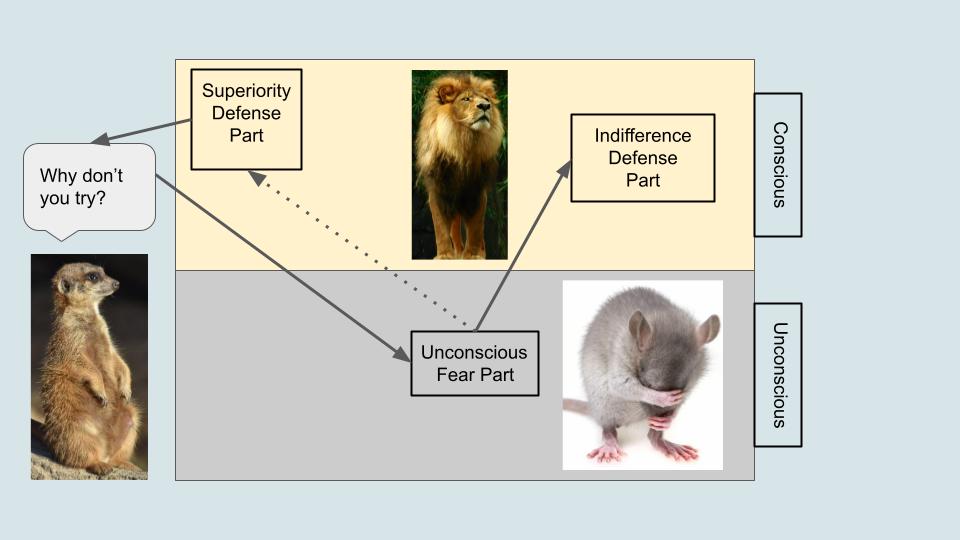 Your parts and their interactions can take over the Whole Self and obscure the (transcendent) Self when the Whole Self starts identifying with the parts. When the (transcendent) Self is unobscured by parts, the Whole Self can act as a witness and a container that enables you to remain objective and regulated, even in highly challenging situations. Function of self The Function of self refers to things happening in the person and out in the world. Functions are processes of actions, beliefs, and defenses. In the Somatic Field, we talk about the Function of self through the concept of the Satisfaction Cycle from Bonnie Bainbridge Cohen’s Body Mind Centering.  These physical actions (to yield, push, reach, grasp, or pull) are metaphors for how we relate to the environment inside and outside ourselves. Each section of the cycle has an action type and beliefs that make the action more or less available to any particular person. Each of these actions can be used as a helpful or unhelpful defense. The satisfaction cycle is only one way to think of the Function of Self. Another version is these three actions in no particular order: reflecting, moving towards/away from the self, and resting or THINK ↔ DO ↔ BE ↔.  Healthy Character Structure (Eudaimonia) vs. an Unhealthy Character Structure (Noseo)
I want to be careful when talking about the “healthy” and “unhealthy Character Structure.” The unhealthy Character Structure emerges for really good reasons initially. The paradox is that it is often healthy to create and spend time in the unhealthy version of the structure of self. Trying to jump into the healthy Character Structure is unadvisable, dangerous, and almost impossible to achieve. If one were to achieve such a seemingly rapid transformation, odds are, it would be superficial and potentially disastrous. If the human psyche changes too rapidly, you can experience states similar to psychosis. This is why genuine therapeutic change at the root of the issue can take years and why most short-term therapy models do not make permanent changes for most people and situations. The unconscious will not allow it. A healthy Character Structure has gratitude and agency built by humility and empowerment (Paul Conti, MD). It becomes harmonious with the (transcendent) Self, creating Eudaimonia. Healthy pursuit is called agency. Agency refers to the ability to act independently and make choices. Gratitude characterizes healthy reflection and rest. Gratitude means being in a state of mind where you can think of all the good things built into life and what others have done for you. Humility is the willingness to see yourself as a part of the whole and to acknowledge that you depend on others. Empowerment means accepting the ability and responsibility to take action in the world. You want a Whole Self who says, “I am here, I can do good things, and I am part of a greater whole (Conti).” An unhealthy Character Structure has avoidance and cynicism caused by disempowerment and grandiosity. It is discordant with the (transcendent) Self, creating Noseo. Avoidance in response to excessive conscious or unconscious confusion, fear, and despair is unhealthy. Avoidance feels relieving in the short term but perpetuates the problem being avoided in the long term. Cynicism is an attitude of negativity and pessimism projected onto the world and people. The cynic separates themselves from others with a grandiose defense, seeing themselves as exceptionally superior or inferior (grandiosity in reverse). They cannot see the gifts of life and the good deeds towards them from others. How to build Eudaimonia? If you know the enemy and know yourself, you need not fear the result of a hundred battles. If you know yourself but not the enemy, for every victory gained, you will also suffer a defeat. You will succumb in every battle if you know neither the enemy nor yourself. - Sun Tsu The Art of War. Swap out “enemy” for environment and “battle” for life challenge from the quote. To build Eudaimonia, you must, above all, get to know yourself. Secondly, you must know the true nature of the world around you as best you can. Being honest with yourself about your own nature and the nature of the world is a painful process initially. Once you have more clarity, you will want nothing more than to continue to refine the accuracy of your understanding of yourself and the world. As you progress on the journey of self-knowledge, you will have to learn your basic nature (your propensities, actions you naturally tend towards) and the collection of habits built on top of it. Your habits form from your basic nature’s interaction with the world around you, which is why life events are crucial to becoming ourselves. Early life events are especially important because early life is when you form your first habits. Those early habits get practiced so much that they become permanent features of your Character Structure. Each habit you acquire is a solution to a regular problem. Habits are not inherently good or bad; they are created to help you survive. Habits either continue to be helpful, or they become unhelpful. You begin to build Noseo if you keep trying to do too many unhelpful habits. You build Eudaimonia when you can adapt your habits as your environmental circumstances change and demand different behaviors from you. As they say in Alcoholics Anonymous, “The definition of insanity is doing the same thing over and over again and expecting a different result.” People get stuck in unhelpful habit loops because of repetition-compulsion and learned helplessness. Repetition compulsion is an unconscious habit performed without thought, like drug addiction. These habits can include trauma reenactments, when you seek out situations that remind you of previous trauma, like getting into abusive relationships as an adult after growing up in an abusive household. In the short term, repeating the pattern decreases anxiety because it's familiar and gives you a sense that you have another chance to understand or master something that previously caught you off guard. Learned helplessness happens when you are wounded so repeatedly in the same way that you grow more familiar and comfortable with that pain than you are comfortable with states of pleasure and well-being. You know you want things to improve but cannot see any way out of your situation. Learned helplessness is psychological blinders that prevent you from seeing other options, even obvious ones. To end cycles of repetition-compulsion and learned helplessness, you must address your trauma wounding. Trauma is anything you have experienced in life that has left its mark on your psyche. Like a physical scar, psychological scars alter the makeup of your Character Structure forever. We can never forget or erase the past, but we can change how we relate to it so that it negatively affects the present as little as possible. Sometimes, it can be as simple as helping the bodymind to realize that the trauma it’s looping on is over now. If you have an ongoing trauma like oppression or chronic illness, you must decide how you will relate to your circumstances. You should not try to “pull yourself up by your bootstraps.” Living in dissociation of your circumstances is not true Eudaimonia. Zenju Earthlyn Manuel's The Way of Tenderness is a fantastic book about remaining tender to ongoing trauma and addressing it in your community, body, and relationships while still carving out the most thriving life possible for your circumstances. You deserve to thrive. Furthermore, and perhaps more importantly, if you are privileged and healthy and you deny the suffering around you, this is also not Eudaimonia. Denial of suffering is persecution. Persecution is an addiction we use to avoid our own trauma and suffering. Rather than address our own traumatized parts, we transfer our trauma onto others. Instead, be honest that structures exist in institutions and the medical field that arbitrarily make life harder for specific groups and act within your sphere of influence to change those structures. Even the smallest contribution to change counts. As you address your trauma, you must also sincerely pursue your chosen goals with flexibility and humility. Conti asks, “Do you take care of yourself? Are you happy you’re here? Do you engage productively in the world?” As you take care of yourself and work to understand the world, you will naturally become humble and empowered to engage productively in the world. You will feel rewarded by your productivity, which causes your sense of agency to increase. You understand that you do not achieve things alone, which increases your gratitude. Endowed with agency and gratitude, you feel happy to be alive, blessed with Eudaimonia. All of this begins with understanding and caring for yourself. There is no “end” to building Eudaimonia. Instead, you learn and enact various processes that are the end in and of themselves. These processes get you through times of the mundane, ecstasy, tragedy, and triumph. They enable you to thrive and, when necessary, survive. Think of the Character Structure as a marble sculpture. You start with a chunk of marble. You begin to chisel a rough shape. Then, most of your time creating the sculpture is spent refining that rough shape. Even when the sculpture is declared “complete,” it still requires protection and restoration from decay and injury. The process is never done. How a Therapist Helps You Build Eudaimonia. You should find your own approach to Eudaimonia. A therapist can help speed and refine your process. Therapists do many things to help, but they primarily do the following: reflect your (transcendent Self), character structure, and function of self back to you so it is easier to see yourself; support you in accurately seeing your environment; identify blocks that you habitually avoid or defend against; and provide interventions that can help those blocks resolve faster and more permanently. You want to make sure you find a therapist that is the right fit for you. Time and time again, it is shown that rapport is the most essential component in an effective therapeutic relationship. Your therapist should:
Having a relationship of rapport with a therapist can be enough to break through old habits and blocks without much fancy footwork from specific types of therapy. When you come to therapy for the first time, you talk about the problems you want to solve. Think of your “problems” like a puzzle or math equation: “I want to get close to people, but simultaneously, I also fear people. I feel lonely because I don’t know how and/or why this happens and, therefore, can’t act differently. I wonder how I will solve this problem.” You seek help from a professional because you hope they can help you see things in yourself you can’t see on your own so that the problems become simpler and, therefore, surmountable. After being in therapy for a while, you feel less overwhelmed and have more of a sense of the consistent problem areas of your life and the sorts of things that help those problems. You still work hard, but the work is simpler. You have the statue's shape and are now in a state of refinement. The math problem metaphor is helpful, but I want to add a caveat. Solving psychological problems can be predictable but not straightforward in the conventional sense. You need simple changes like gratitude journaling, adding movement activities to your life, examining your thought patterns, etcetera, but you also need more intangible interventions like learning to feel your feelings fully and understanding your parts. The intangible pieces are the daimon of Eudaimonia. This is where a good therapist is particularly beneficial. Connecting to your (transcendent) Self is an art and a practice. I can describe the art to you as I understand it, but you must become the artisan of your own psyche. A good therapist does not only teach you; they midwife your sage within. The aim of therapy is Eudaimonia, to harmonize your Whole Self and Character Structure to the (transcendent) Self. There are many practical avenues to achieving this harmony, but there are also many mysterious components to the process. You want a therapist who has been trained in both the practical and the mystery and who has done their own work themselves. This is the most important thing for therapy, more than any particular type of therapy. As an adult, you also must take full responsibility for building your Eudaimonia while also considering your circumstances (chronic illness, oppression, your particular life situation, etc.). This is the most important thing for you as an individual. There is much more to say about building Eudaimonia in a therapeutic relationship than this essay covers. I have done my best to bring forward the foundational aspects of this pursuit. |
AuthorProsopon Therapy Archives
April 2024
Categories |
||||||||||||||
 RSS Feed
RSS Feed