|
The Satisfaction Cycle and Sensitivity Cycle are common frameworks used in somatic therapy. The Satisfaction Cycle reflects how engaging in the environment shows up developmentally and somatically and discusses ways that developmental wounding disintegrates these five actions. The Sensitivity Cycle provides a similar schema and exploration but focuses on how direct action differs from adapted indirect action. Each schema discusses ways barriers or blocks can appear at each stage of the cycle and recognizes that each barrier and block comes from some form of wounding and subsequent adaptation. 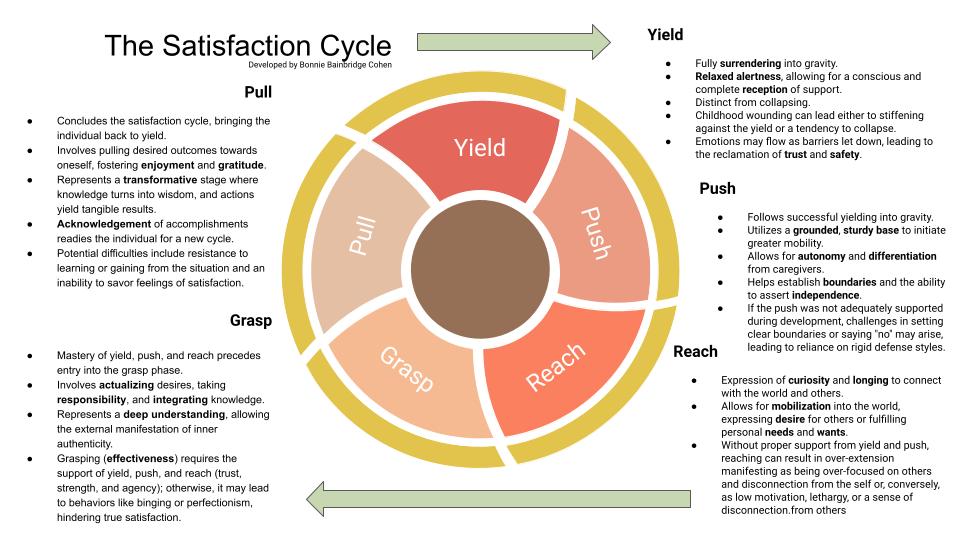 The Satisfaction Cycle from Body Mind Centering The Satisfaction Cycle is a guiding principle within Body Mind Centering, intertwining physical movements with the developmental stages that shape our early years. Rooted in the simplicity of infancy, this cycle manifests through five core movements: yield, push, reach, grasp, and pull. In this exploration, we note key points of each phase and contemplate its impact on our internal experiences as adults. YIELD: Receiving Support with Presence Yielding is relaxing into gravity and the support of the chair, bed, or ground as you sit, lay down, or stand. Like a loved infant, you fully trust what holds you, melting into your container. You are present but your awareness is soft, oceanic, and expansive. You consciously enjoy this held feeling with a sense of gratitude. You do not feel stuck, trapped, or frozen as in a collapse or resistance state. Rather, you feel that you can rest and connect here until you feel ready to use this surface as a sturdy base from which to launch in a graceful, integrated way. Without the trust of the yield all other movements are compromised.
PUSH: Grounding, Knowing and Asserting the Self Pushing refers to how the body interacts with gravity and the sturdy base. It involves pressing body parts into supporting surfaces, which creates a compression in the tissues, bones, and joints. Pushing represents the internal awareness of ourselves and asserts our separate sense of self, laying the groundwork for setting boundaries. Lack of boundaries or overly rigid defenses can emerge if independence was either rushed or thwarted.
REACH: Toward Space, Levity, and Desire Reaching is the body’s relationship to space. Reaching brings our attention to what is external to the body and the self. It uses the support of the sturdy base and the strength of the push to create lightness and buoyancy in body parts as they extend out into the world. Reaching lengthens muscles and tissues, supporting the ability to say "yes" and move toward desires. Without yield and push (trust and strength) the reach can become frantic, compulsive, restricted, or confused. Examples of this are people pleasing, not pursuing your own wants and needs, feeling unable to identify someone you want to connect with, and not knowing how to take initiative.
GRASP: Actualizing Desires, Learning, and Achieving Goals Having mastered yield, push, and reach, we enter the grasp phase. This stage involves actualizing our desires, taking responsibility, and integrating knowledge. It symbolizes a deep understanding that allows us to actualize our inner authenticity in the external world and marks part one of the culmination of the satisfaction cycle. Without the support of yield, push, and reach (trust, strength, and agency) grasping (effectiveness) is elusive. In that case, grasping can become like binging food or television long after satiety, or neurotic perfectionism where one never allows the project to be done, or getting the promotion but avoiding the learning and responsibility that goes with it, or reading a lot of self-help books but never putting the the advice into practice, or receiving a proper apology with a behavior change but continuing to resent the person who apologized.
PULL: The Moment of Transformation The pull phase completes the cycle, bringing us back to yield. As we pull what we desire towards us, we enter a state of enjoyment and gratitude, reflecting on our achievements. Pull is a stage of transformation. Knowledge becomes wisdom, responding becomes an outcome, food is assimilated into the body, work becomes a product, an apology becomes a repair, a promotion becomes a fulfilling wonderland of challenge and growth. Accepting what has been received or accomplished readies us for a new cycle or interest.
Thus the action yield, push, reach, grasp, and pull work together building a foundation of trust upon which flexible strength can develop, which lends itself to the lightness of desire that ignites our effective action in the world that provides results that foster enjoyment and gratitude which in turn creates more trust and stability. Mastering the Satisfaction Cycle create a positive feedback loop that leads to fulfillment, connection, and abundance. 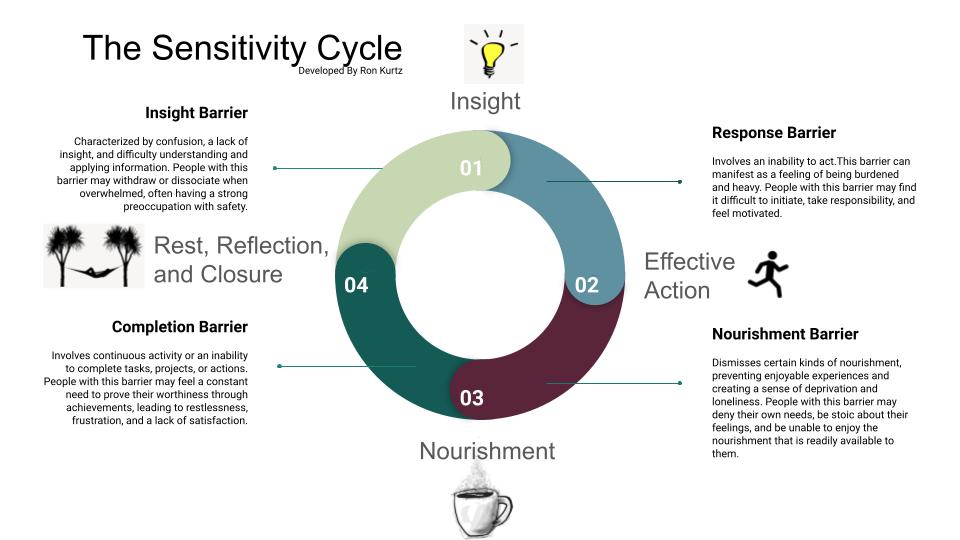 The Sensitivity Cycle and the Barriers to Aliveness
Invented by Ron Kurtz, the Sensitivity Cycle is a central theory of the Hakomi Method, attempting to explain the intricate ways in which individuals perceive, process, and navigate their experiences. When the sensitivity cycle functions optimally it presents as a harmonious interplay of four key elements.
A seamless synergy of these four elements cultivates a sense of flow in one's life. However, due to developmental wounding, trauma, and the adaptations that follow, there exists the potential for getting "stuck" in unhealthy patterns or situations that can be thought of as barriers at one or more of the stages of this cycle.
Regardless of the specific barrier type, a core belief persists that you cannot directly ask for or obtain what you want or need. This deeply embedded belief that came from long ago, usually childhood, influences your ability to act in relationships and the world. Instead of being direct, you develop complex strategies aimed at fulfilling your wants or needs. However, despite your efforts, these strategies consistently fail to get you what you want and need, leading to ongoing frustration, disappointment, and deprivation.
0 Comments
From my perspective, a cognitive distortion arises when a “part” or subpersonality is activated and in distress. A Part is any subpersonality that arises that is not the “compassionate witnessing observer” (CWO). People sometimes refer to their “parts” as sides, modes, etc. of themselves (“I have a dark/wild/naive/youthful/serious side,” “I can really get into hyperfocus mode,” “part of me just loves to dance and I have to take him out to the honky-tonk,” etc.)
The “compassionate witnessing observer” (CWO) is called many things by many spiritual and therapeutic traditions. This is what I choose to call it. Qualities of the CWO include, objectivity, seeing the “good” in everything and everyone but also recognizing when a “good” being is not acting in the best interest of itself or others usually because of confusion. The CWO feels settled and self-assured, calm patience, wholeness, comfort with awareness and presence, and more. When a part is present it does not necessarily mean that the part is in distress. When someone feels distress, however, a part is always present and contains the distress. This is ok, expected, and particularly functional when the part is also connected to the CWO. When the part is not connected to the CWO, is when larger problems can occur. Whether or not the part is connected to the CWO, if the part is in distress, it is likely that the part is embodying a cognitive distortion. A cognitive distortion is when someone's thinking does not align with reality and what someone can reasonably know about reality. Each distortion arises in response to a body state that emerged as a reactive adaptation to the environment and produces a responding body state that further attempts to adapt usually to a suboptimal situation. All body state responses are unique to the individual. As you read through these, notice what your body does. Stick with sensation (tingly, hot, metallic, collapsed, watery, foggy, etc.) rather than story or emotional words. Do your best to stay in touch with your CWO. If you have not had a direct experience with your CWO, that’s ok. However, you are more likely to become triggered, defensive, activated, or have some kind of difficulty in general as you read and feel through this list. Stop the exercise if you reach a limit. All-or-Nothing Thinking (Black-and-White Thinking): Seeing situations in extremes, without recognizing middle ground or shades of gray. Overgeneralization: Drawing broad conclusions based on limited evidence, often making predictions about future events based on a single negative experience. Filtering (Selective Abstraction): Focusing exclusively on the negative aspects of a situation while ignoring any positive elements. Jumping to Conclusions:
Personalization: Blaming oneself for external events or circumstances beyond one's control, or attributing external events to personal actions when there is no evidence for such a connection. Should Statements: Setting rigid and unrealistic standards for oneself or others and feeling guilty or upset when these standards are not met. Labeling and Mislabeling: Assigning global, negative labels to oneself or others based on errors or mistakes, rather than recognizing the specific behavior. Emotional Reasoning: Assuming that because one feels a certain way, the feelings must be accurate reflections of reality. Discounting the Positive: Minimizing or dismissing positive experiences, qualities, or accomplishments, often attributing them to luck rather than personal effort. Mind Bluffing: Believing negative thoughts without questioning their validity, taking them at face value. Control Fallacies:
You made it to the bottom of the list! Take a movement, breathing, water, or presence break. Come back to center. Reconnect to your CWO. What did you learn about yourself? 2/18/2024 Object Relations Theory: A Classical Conceptual Foundation for Understanding Modern Attachment TheoryRead NowI am adding a discussion of Object Relations Theory to my blog because it is a theory that has greatly influenced my work. In my opinion it is the beginning of the discussion of attachment and still provides a worthwhile perspective to the modern clinician or informed client despite being a classical theory.
At the end of this article I lay out Mahler’s stages of separation in early life. I do this because the nature of the primary wounding in the client can often be located within one of these stages. Knowing at what stage the client is wounded is useful because the way I as the therapist behaves toward the client is different depending on the wound stage. Object Relations Theory is a psychoanalytic theory that focuses on the way individuals relate to others, particularly in the context of interpersonal relationships. Developed within the psychoanalytic tradition, this theory departs from Freudian drive theory, emphasizing the importance of interpersonal experiences and relationships in shaping an individual's psychological development. The term "object" in Object Relations Theory does not refer to inanimate objects but rather to significant people (objects) with whom an individual interacts, such as parents, caregivers, or other important figures. The theory suggests that early relationships, especially with primary caregivers, play a crucial role in the formation of an individual's mental representations or "internal objects." Key concepts in Object Relations Theory include: Internal Objects: Mental representations of others that influence how individuals perceive and interact with people in their lives. These internal objects are shaped by early caregiving experiences. Attachment: Object Relations Theory is closely related to attachment theory, emphasizing the impact of early attachment experiences on emotional and relational development. Transference and Countertransference: These concepts involve the projection of feelings and expectations onto others (transference) and the emotional reactions of the therapist (countertransference) in a therapeutic relationship. Splitting: The tendency to perceive people or situations as all good or all bad, reflecting a lack of integration of positive and negative qualities in others. Introjection: The process of internalizing external objects, incorporating aspects of others into one's own sense of self. Object Relations Theory has been influential in the field of psychotherapy, especially in psychodynamic and relational approaches. Therapists utilizing this perspective aim to explore and understand how past relationships and internalized objects impact a person's current emotional and relational functioning. Here is a list of some key figures associated with Object Relations Theory and the nature of their contributions: Melanie Klein: A pioneering psychoanalyst who made significant contributions to Object Relations Theory. She focused on the early stages of infant development and the impact of internalized objects on psychological functioning. Anna Freud: Continued her father’s work by emphasizing the impact of early childhood experiences, particularly the mother-infant relationship, on the formation of internalized mental representations and object relations in individuals Donald Winnicott: Known for his work on object relations, transitional objects, and the "good enough mother" concept. Winnicott emphasized the importance of the mother-infant relationship in shaping the individual's sense of self. Ronald Fairbairn: Contributed to the development of Object Relations Theory, emphasizing the role of internalized objects and the impact of early relationships on personality development. Wilfred Bion: Extended Object Relations Theory by introducing concepts like "container-contained" and "alpha function." Bion explored the emotional and cognitive aspects of the mother-infant relationship. Margaret Mahler: Known for her research on infant development and separation-individuation processes. Her work has been influential in understanding the early formation of object relations. Harry Stack Sullivan: While not exclusively an Object Relations theorist, Sullivan's interpersonal theory influenced later developments in Object Relations Theory. He emphasized the role of interpersonal relationships in shaping personality. Otto Kernberg: Integrated Object Relations Theory with psychoanalytic concepts and made contributions to understanding personality disorders, particularly focusing on borderline personality organization. Heinz Kohut: Developed Self Psychology, a branch of Object Relations Theory, focusing on the role of self-objects and the formation of a cohesive sense of self. D.W. Winnicott: A psychoanalyst who extended Winnicott's ideas and made further contributions to Object Relations Theory, particularly in the areas of play and creativity. Margaret Mahler, a psychoanalyst and researcher, proposed a developmental model known as the Separation-Individuation theory within the context of Object Relations. This theory outlines stages in the early development of infants as they form a sense of self and relatedness to others. The key stages in Margaret Mahler's Separation-Individuation theory are:
Margaret Mahler's stages of development emphasize the gradual process of separation and individuation, with a focus on the evolving relationship between the infant and the primary caregiver. If there is a major disruption at one or more of these stages, the likelihood of maladaptation increases and shows up in a manner that is associated with the stage at which the disruption occurred. This is useful to know as a clinician or client because the solution to the wound can be found in the task of the stage at which the wound occurred. This notion that the wound contains the antidote is common across psychological theories and, in my experience, pans out in the actual practice of psychotherapy.
What is Past Reality Integration (PRI)?
PRI, created by Ingeborg Bosch, operates on the assumption that emotions and behavioral patterns impacting our daily lives are rooted in old traumas from our early years, often unbeknownst to us. Whether grappling with depression, burnout, anxiety, panic attacks, addiction, eating issues, or relationship challenges, PRI posits that the origin of these problems lies in past experiences, veiling the residual pain from that time. In PRI therapy, your therapist guides you to apply PRI techniques independently based on your specific concerns, a process established during an intake interview. Through careful observation and utilization of the PRI model, which elucidates the workings of the brain, you gain deeper insights into your emotions and defenses. The therapeutic process involves consciously halting habitual behaviors to access latent, unconscious feelings linked to your past. The ultimate goal is not to perpetuate the experience of old pain but to progressively live without unnecessary challenges and defenses. PRI therapy enables you to swiftly recognize and dismantle activating behaviors, allowing you to experience the present unburdened and fostering authentic connections with yourself and your environment. The Handout The handout available for download at the top of this webpage lists off the defenses people commonly use to protect against perceptions of abandonment, rejection, and neglect. On the first page, you'll see each defense listed and the antidote to it right after. Below the defense-antidote you will see the "narrative" of the defense or the thoughts that go with it. On the second page, you will see the PRI model of a trigger. At the bottom of the second page you see on the left the trigger getting integrated and on the right the trigger getting suppressed and filed back into the unconscious. A defense mechanism is a subconscious psychological strategy employed by individuals to cope with and manage emotions, particularly anxiety or stress, by protecting themselves from thoughts, feelings, or impulses perceived as threatening or distressing. These mechanisms operate outside of conscious awareness and are aimed at maintaining psychological balance and protecting self-esteem. Introduced by Sigmund Freud and further developed by other psychologists, defense mechanisms include many different processes, including the ones listed below. While these mechanisms can be adaptive in moderating emotional distress, their overuse or misuse may lead to maladaptive coping strategies, hindering personal growth and well-being.
Repression: Unconsciously forgetting or blocking out unpleasant memories or thoughts. Denial: Refusing to acknowledge the existence of something distressing or threatening. Projection: Attributing one's own unacceptable thoughts, feelings, or motives to others. Displacement: Redirecting emotions or impulses from their original source to a less threatening one. Sublimation: Transforming socially unacceptable impulses or urges into socially acceptable actions. Rationalization: Offering logical or reasonable explanations for behaviors or thoughts that are actually driven by irrational motives. Regression: Reverting to an earlier stage of psychological development in response to stress or conflict. Reaction Formation: Expressing the opposite of what one truly feels or thinks, often as a defense against unacceptable impulses. Intellectualization: Dealing with emotional conflicts or stress by focusing on abstract or intellectual aspects. Suppression: Consciously choosing to not think about or dwell on certain thoughts or feelings. Undoing: Engaging in behavior to counteract or "undo" guilt or anxiety resulting from unacceptable thoughts or actions. Identification: Associating oneself with someone or something in order to enhance self-esteem or reduce anxiety. Fantasy: Creating an imaginary world to escape from or compensate for perceived deficiencies in reality. Compensation: Overachieving in one area to make up for perceived failures or shortcomings in another. Splitting: Viewing people, situations, or oneself in extremes of either all good or all bad, to avoid the anxiety of ambivalence. Somatization: Expressing emotional distress through physical symptoms or ailments. Acting Out: Engaging in impulsive or inappropriate behavior as a way of expressing unconscious emotions. Humor: Using humor as a defense mechanism to cope with distressing situations or emotions. Sour Grapes: a cognitive strategy in which individuals, unable to attain something they desire, devalue or dismiss the desired object or goal as unimportant or undesirable to ease the emotional impact of unmet needs. Selective Forgetting: "Choosing" to remember only certain details of an event while forgetting others to protect oneself from discomfort. Isolation of Affect: Separating feelings from ideas and events, dealing with emotional aspects in a detached and intellectualized manner. Compartmentalization: Separating conflicting thoughts or emotions into separate compartments to avoid internal conflict. Minimization: Downplaying the significance of one's thoughts, feelings, or actions to reduce anxiety or guilt. Idealization: Seeing someone or something as perfect, admirable, or superior as a way to avoid dealing with negative feelings. Withdrawal: Physically or emotionally removing oneself from a situation to avoid potential stress or conflict. Passive-Aggression: Indirectly expressing hostility or anger through passive means rather than directly confronting the source. Sarcasm: Using humor or irony to mock or convey contempt in a way that masks true feelings. Autistic Fantasy: Retreating into a rich fantasy life to escape from reality and cope with emotional stress. Projective Identification: Projecting positive or negative thoughts or feelings onto another person and simultaneously reacting with the projected material as if it now belongs to the other person. Self-Serving Bias: Attributing positive events or successes to one's own character while attributing negative events or failures to external factors. Spiritual Bypassing: Using spiritual beliefs or practices to avoid dealing with unresolved psychological issues. Compulsive Behavior: Engaging in repetitive, ritualistic actions to alleviate anxiety or prevent a feared event from occurring. 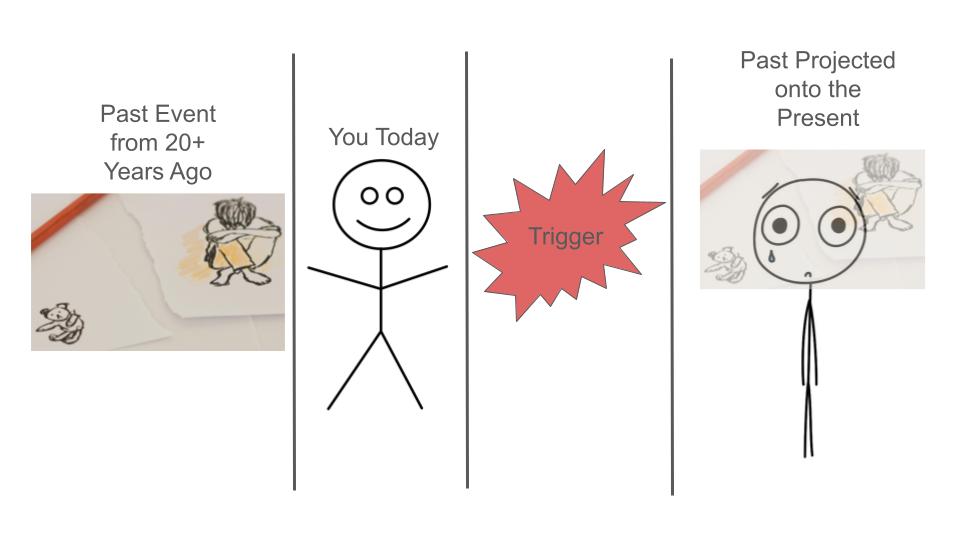 How does getting "triggered" work?
Trigger Logic: this refers to the the thought pattern related to maintaining the intensity and "flavor" of the trigger. When in the process of a trigger, we can feel like it is of the utmost importance to maintain the triggered state; that to let it go would compromise our integrity, safety, or goal in the moment. The thoughts can say to us that it is impossible to regulate. To even think of regulating can feel threatening, insulting, or shaming. It Just Feels So Real: The reason its hard to "reason" with a trigger is because your body really feels like its in the original past event while your mind does not have the sensation of remembering. So you are actually feeling the past but absolutely cannot distinguish it from the present. In our example, the loss of the keychain object feels like the forced removal of the stuffed animal when you were a little child. The self attack you engage in is the defense you used as a child to deal with the wound created by the misattuned parent. When the stuffed animal was taken away, your little body went into chaos. You didn't understand what was happening and blamed yourself, because that is what little children do to maintain the notion that their caregivers are "good, reliable, and worthy of trust." It is safer for a child to think that they are the problem rather than the adults because they rely on the adults for survival. So, when you are triggered, you essentially "forget" you are an adult and feel like a threatened child, teenager, or some other past disempowered version of yourself. You experience that past version in your body and you feel like that version is you in the here and now, even though it is not, in fact, you currently. Regulation: Its Not So Easy. Just because there is a thought component to trigger logic does not mean that it is easy to "just regulate" in the moment. Regulating take a ton of awareness and practice. People who have been able to practice genuine regulation are lucky, privileged, and hard-working because genuine regulation practices are hard to come by and, at times, hard to learn. Once someone understands how to regulate and their particular needs regarding regulating, the process can become quite simple. The road to simplicity can be a long and harrowing one, however, with many opportunities for illusions, mysteries, and traps along the way. How do I learn to regulate?
How do I know that I am regulating and not dissociating or coping with compartmentalization? In essence, you will be able to assess the objective magnitude of an event in terms of its level of threat towards you and others. You will be able to recognize that most unpleasant events are uncomfortable and inconvenient but are not emergencies or a sign that either you or the world are completely awful. Your emotions will serve as trustworthy messengers rather than threatening energies that totally overwhelm you. You will be able to think and feel at the same time and be able to choose a course of action that is in your and other's best interest. Survivor Bias
I wanted to address survivor bias because I often talk about how to achieve positive outcomes in mind-body health care. I felt it would be unethical not to mention the reality that not everyone heals. It is so tempting to stay focused on those who heal and how they did it, but ultimately, it can be really hard to discern what caused the healing, especially because I tend to advocate that my clients pursue a multidisciplinary route to healing. Privilege It should also be noted that there is a lot of privilege at times in being able to pursue a multipronged healing approach. I personally sit with grief that transformation is not available to all who desire it. Here are some of the way that survivor bias interferes with our ability to better understand the crux of healing in both mainstream and alternative healthcare: Survivor Bias in Mainstream Healthcare Survivor bias in health outcomes refers to the distortion that can occur when analyzing data or drawing conclusions about health based only on individuals who have survived or reached a certain point in a study, treatment, or condition. This bias arises when individuals who did not survive or dropped out of the study are not included in the analysis, leading to an incomplete and potentially misleading understanding of health outcomes. Here are a few examples to illustrate survivor bias in health outcomes: Clinical Trials: If a clinical trial only reports the outcomes of participants who completed the study and ignores those who dropped out due to adverse effects or lack of improvement, there may be a biased representation of the treatment's effectiveness. Including only "survivors" in the analysis can overstate the positive effects and underestimate potential risks. Longitudinal Studies: In studies tracking the health outcomes of a particular population over time, survivor bias can occur if the analysis is based solely on individuals who have reached a certain age or milestone. This may lead to an overly optimistic view of the population's health, as those who experienced negative health outcomes or premature death are not considered. Disease Registries: When compiling data from disease registries or databases, survivor bias can occur if only individuals who are still alive or actively seeking treatment are included. This might lead to an underestimation of the severity of the disease or the effectiveness of certain treatments. Observational Studies: In observational studies where individuals self-select into treatment groups, survivor bias may occur if only those who respond positively to a particular intervention continue to participate or report their outcomes. This could create a falsely positive impression of the intervention's efficacy. To address survivor bias in health outcomes, researchers need to consider the entire population under study, including those who did not survive or dropped out. Analyzing complete datasets allows for a more accurate assessment of the factors influencing health outcomes and helps avoid drawing conclusions based solely on individuals who have "survived" a particular point in the process. Survivor bias in Alternative Health Care: Survivor bias can also be relevant when evaluating health outcomes in the context of alternative healthcare practices. In this context, survivor bias may manifest in various ways, potentially affecting the perception of the efficacy and safety of alternative treatments. Here are a few scenarios where survivor bias might be observed in alternative healthcare: Self-Selection Bias in Testimonials: Individuals who have positive experiences with alternative healthcare treatments may be more inclined to share their success stories or testimonials. This self-selection bias can create an unrepresentative sample, as those who did not experience positive outcomes or had negative reactions may be less likely to report their experiences. Online Communities and Forums: Discussions in online health forums or communities may primarily involve individuals who have had positive experiences with alternative treatments. Negative experiences or lack of efficacy might be underrepresented, leading to a skewed perception of the success rates of these treatments. Long-Term Follow-Up: Alternative healthcare practices often lack rigorous long-term studies and follow-up assessments. If individuals who initially report positive outcomes are followed up, while those who did not experience benefits or faced adverse effects drop out of follow-up studies, survivor bias may lead to an overestimation of treatment success. Exclusion of Unsuccessful Cases in Research: Some alternative healthcare studies may selectively report positive results and exclude cases where the treatment did not work or caused harm. This can lead to an inflated perception of the overall success of the treatment. Underreporting of Adverse Events: Individuals who have adverse reactions to alternative healthcare treatments may be less likely to report these events, especially if the treatment is perceived as unconventional or not widely accepted in mainstream medicine. This can result in an incomplete understanding of the potential risks associated with alternative therapies. To mitigate survivor bias in alternative healthcare, it's essential to approach the evaluation of treatments with a critical and evidence-based perspective. Researchers and practitioners should strive to collect comprehensive data, including both positive and negative outcomes, and conduct well-designed studies that account for potential biases. Additionally, individuals seeking alternative healthcare should be aware of the importance of reporting both positive and negative experiences to contribute to a more balanced understanding of the treatments they explore. Humility and Balance In acknowledging the reality of survivor bias, it's crucial to foster a compassionate and honest dialogue about the complexities of healing in both mainstream and alternative healthcare. While we often share success stories and pathways to positive outcomes, it's equally important to recognize that not everyone's journey leads to healing. This acknowledgment doesn't diminish the value of those who find transformation but instead invites us to approach discussions with humility and empathy. Healing is multifaceted, and the pursuit of well-being is often influenced by various factors, including access to resources and personal circumstances. As we delve into the challenges posed by survivor bias, we're presented with an opportunity for growth and a commitment to understanding health outcomes more comprehensively. By encouraging a transparent and inclusive approach in research, we can navigate the complexities of both mainstream and alternative healthcare, ensuring that the experiences of all individuals, regardless of their outcomes, contribute to a more nuanced and balanced understanding of health and healing. Challenges in Implementing Change
I’ve worked with some really challenging psyches, especially my own. I’ve seen mind boggling transformations. I’ve also seen people languish for years in the doldrums or agony while wondering why transformation seems out of reach for this person and not for another. The interventions we offer are hugely important in creating the change, but if the seed of change is planted on unprepared soil, very little or nothing is likely to grow. The person receiving the intervention must know already or learn how to accept change once it has been made. This is a necessary condition that is often overlooked by professionals when prescribing special diets, meditation plans, and even surgeries and medicine. If a client does not know how to change and be different, I believe the likelihood of an intervention working is impacted. Upper Limits Problem This is something akin to the upper limits problem. The "upper limits problem" refers to a psychological phenomenon where individuals set self-imposed ceilings on their achievements or capabilities, often without realizing it. People may unknowingly sabotage their own potential by subconsciously adhering to these limits, which can hinder their progress and prevent them from reaching their full potential. Overcoming the upper limits problem requires self-awareness, introspection, and a willingness to challenge ingrained beliefs and behaviors in order to break through these artificial barriers and unleash one's true capabilities. The willingness necessary to change may be hard won, however, depending on how dysregulated a person’s nervous system is. The Resourcing Phase This is why the “resourcing” phase is so crucial. The resourcing phase in trauma therapy means training the nervous system to be regulated enough for trauma processing. That does not mean “applying” regulation techniques like breathing, positive thinking, stretching and so on. Rather that means validating pain in the client in a specific way that enables the resources to emerge on their own. Due to the non-linear nature of this process and the varieties of nervous system presentations, this phase can take a long time or be the only phase that a client ever works on. I really want to believe that nervous system healing is possible for everyone, barring extreme damage to the system. I hope that as we continue to learn more about the nervous system that we get increasingly better and efficient at helping people make lasting changes despite innate challenges. Cognitive Dissonance and Belief Systems This week in my practice I became more aware of how cognitive dissonance presents in clients who seem to experience better psychological states and then fall back into old patterns and systems of belief over and over again. It is so important to note that “just changing your belief system” is not a thing. Occasionally we see a radical change in belief system but instances such as these are outliers and not the norm. Beliefs are embodied and the embodied experience of a belief must change along with the “words in the head” (thoughts). Typically I see progress being made in clients like an inchworm, to put it in an overly simplistic way. Half of them get to a new state then the other half catches up and on and on. Cognitive dissonance is a psychological theory developed by Leon Festinger in 1957. It refers to the discomfort or mental tension that a person experiences when they hold two or more conflicting beliefs, attitudes, or values simultaneously, or when their behavior conflicts with their beliefs or values. The key idea behind cognitive dissonance is that individuals strive for internal consistency in their thoughts, beliefs, and attitudes. When inconsistencies arise, they are motivated to reduce the discomfort by changing one of the conflicting elements. This can happen through various means, such as changing one's beliefs, acquiring new information to support existing beliefs, or minimizing the importance of the conflict. For example, if someone is aware that smoking is harmful to health but continues to smoke, they may experience cognitive dissonance. To reduce this discomfort, they might downplay the risks of smoking, convince themselves that they have other healthy habits, or find other ways to justify their behavior. Cognitive dissonance theory has been widely used to explain various psychological phenomena, including attitude change, decision-making, and rationalization of behavior. Addressing Cognitive Dissonance Addressing cognitive dissonance involves acknowledging and resolving the conflicting beliefs, attitudes, or behaviors causing discomfort. Here are some strategies to directly address cognitive dissonance: Awareness: to become aware of the cognitive dissonance is half the battle. Furthermore, acknowledging and admitting that one is in a cognitive dissonance dynamic invites intentionality rather than reactivity when it comes to addressing the dissonance. Somatic Exploration of Beliefs: this goes along with awareness. Beliefs are not just in the thoughts. Beliefs express through the body. If I believe that I am bad, I may have a collapsed posture. If I believe that I am worthy of love, my body may take a relaxed attitude. Seek Information: I may need to learn more about each conflicting side of the dissonance. In this context, I may need to learn more about the origin of the limiting belief in my life. In turn, I may also need to learn more about the more helpful mindset before my intellect feels comfortable with going through the change process. Explore the Golden Shadow: unhelpful beliefs are often in “parts” or subpersonalities that we have disowned. The best course of action in dealing with parts is to acknowledge that the now unhelpful belief was actually beneficial at one time and brought many gifts with it. You can then invite the part to transform and take on a new “job,” thereby more fully expressing its innate gifts. Case Example: Sonia's Struggle with Self-Worth and Self-Care Sonia, a 40-year-old executive, sought therapy to address persistent feelings of low self-worth. Despite her professional success, she struggled with a deep-seated belief that she was not worthy of care and attention, leading to challenges in implementing a self-care routine. Making time for herself brought up an unbearable feeling of friction and a panic like feeling in her body. Background: Sonia's childhood was marked by high expectations from her parents, conditioning her to believe that her value was contingent on achievement. This belief persisted into her adult life, impacting her relationships and, most notably, her ability to prioritize self-care. Presenting Issues: In therapy, Sonia expressed feeling overwhelmed by work demands and the constant need to prove herself. Despite recognizing the importance of self-care, she found it challenging to implement and sustain a routine due to an underlying belief that taking time for herself was undeserved. Pressure was mounting for her to resolve this conflict because she was beginning to develop significant digestive issues that were interfering with her ability to function. Therapeutic Process: Awareness Stage: Sonia, with the support of her therapist, became aware of the cognitive dissonance between her acknowledgment of the importance of self-care and her ingrained, felt-sense belief that she didn't deserve it. This dissonance triggered anxiety and guilt whenever she attempted self-care activities. Somatic Exploration of Beliefs: Through therapeutic conversations, Sonia explored the origins of her belief system and how that was showing-up in her body. She discovered that her worth had become tied to external validation, and any focus on self-care stirred feelings of guilt and impending inadequacy. When engaging in self-care shoe could not relax her body and take in the nourishing effects of self-care. Seeking Information: Sonia engaged in educational sessions with her therapist to understand the psychological and physiological benefits of self-care. Sonia values scientific data, so her therapist provided articles that satisfied Sonia’s intellect. This information highlighted how her negative beliefs about self-worth came from her attempts to survive her past relationship with her parents and did not make sense as a useful mode of function in her life now. Cognitive Dissonance Challenge and The Golden Shadow: Sonia faced the challenge of actively challenging her belief system. As she started incorporating small self-care practices, such as walks in nature and setting time boundaries at work, she experienced internal resistance in the form of feelings of guilt and anxiety. Sonia practiced staying with the physical sensations of her resistance as she took steps to care for herself anyway. Sonia was able to validate how useful the adaptation of self-denial was early on in her life and discovered that this “part” that self denies holds her intuitive awareness of her want and needs and how to flow through her life addressing those wants and needs while also staying on top of responsibilities and goals. Resolution and Integration: Over time, Sonia worked on reframing and reembodying her beliefs about self-worth. She discovered that her down time and boundaries not only did not detract from her value, rather, they enhanced her ability to be efficient and creative at work. Furthermore, the backlash she expected from colleagues never came and Sonia realized that people around her approved of her prioritizing herself. The therapist guided her in developing a self-compassionate narrative and understanding that self-care was not only deserved but crucial for her overall well-being and, secondarily, her performance as a worker. Outcome: As Sonia persistently confronted her cognitive dissonance, she began to see positive changes. The implementation of a self-care routine, initially met with inner conflict, became more natural. Sonia reported feeling more in flow, resilient to work stress, and, most importantly, a growing sense of embodied self-worth detached from external achievements. Closing thoughts: This case highlights the intricate relationship between self-worth and the ability to prioritize self-care. Through somatic exploration, embodied parts work, gentle exposure therapy, Sonia experienced organic cognitive restructuring and successfully navigated the cognitive dissonance, fostering positive changes in her beliefs and daily practices. You can see why it is hard for individuals to make big changes at times. An important stage of change I am noticing in my own processing is the need to intentionally create integration time after a big session. It goes like this: I work on a big wound, the session ends on a note of care, love, and self-compassion, and then I am facing the unknown. My personality now has the opportunity to update, but I must make space for the unknown. There is a tendency for humans to fill in the unknown with old stories, interpretations, and explanations. For my personality to really update, I have to know what the unknown feels like and intentionally stay there for awhile with curiosity about what will come through next. I allow my personality to update spontaneously rather than imposing an ideal created by my thoughts. In this way, I consciously confront the upper limits problem and cognitive dissonance to that the new can emerge. If you are new to the mental health treatment world, you may feel confused and overwhelmed by the different letters at the end of practitioners names. Here is a glossary of mental health practitioner types and licenses.
Psychiatrist: A medical doctor (MD) or doctor of osteopathic medicine (DO) specializing in the diagnosis, treatment, and prevention of mental illnesses. Psychiatrists can prescribe medication. Psychologist: A professional with a doctoral degree (Ph.D. or Psy.D.) in psychology, trained to diagnose and treat mental health disorders through therapy and counseling. Licensed Professional Counselor (LPC): A mental health professional with a master’s degree in counseling or a related field. LPCs provide therapy and counseling services to individuals, couples, and families. Clinical Social Worker (LCSW): A licensed social worker with a master’s degree in social work and specialized training in clinical practice. LCSWs offer therapy, counseling, and support services. Marriage and Family Therapist (LMFT): A mental health professional with a master’s or doctoral degree in marriage and family therapy. LMFTs specialize in working with couples and families to address relationship issues. Psychotherapist: A generic term for professionals who provide talk therapy to address emotional and psychological issues. This term can encompass psychologists, social workers, counselors, and psychiatrists. Psychiatric Nurse Practitioner (PMHNP): A nurse practitioner with specialized training in psychiatry. PMHNPs can assess, diagnose, and treat mental health disorders, including prescribing medication. Substance Abuse Counselor/Licensed Addiction Counselor (LAC): A professional trained to help individuals struggling with substance abuse and addiction. They may hold various degrees, including LPC, LCSW, or specific certifications. Supervisor: A counseling supervisor is an experienced and credentialed professional who provides guidance, oversight, and support to counselors-in-training or practicing counselors to enhance their clinical skills, ethical conduct, and professional development. Milieu Therapist: A therapist who works within a therapeutic environment or community setting, actively shaping the therapeutic milieu to facilitate positive social interactions and promote the well-being of individuals receiving mental health services. Group Counselor: A professional who facilitates therapeutic sessions with a group of individuals, fostering mutual support, communication, and personal growth within the group dynamic. Couples Counselor: A professional who specializes in providing therapy and guidance to couples, assisting them in resolving conflicts, improving communication, and enhancing their relationship. Case Worker: A professional who assesses, plans, coordinates, and advocates for the services and resources needed by individuals or families to address their specific needs and improve their overall well-being. Sex Therapist (CST): a specialized mental health professional who helps individuals and couples address and navigate issues related to sexuality, intimacy, and sexual health through counseling and therapeutic interventions. Sex Addiction Therapist (CSAT): a mental health professional who specializes in assisting individuals with compulsive sexual behaviors, employing therapeutic interventions to address and manage issues related to sex addiction. Art Therapist: A mental health professional who uses art-based interventions to help individuals explore and express their emotions. Art therapists may have degrees in art therapy or related fields. Music Therapist: A therapist who uses music-based interventions to address emotional, social, and cognitive issues. Music therapists may have degrees in music therapy or related fields. Behavior Analyst: A professional trained in applied behavior analysis (ABA) to assess and address behavioral issues, often working with individuals with autism spectrum disorder or developmental disabilities. “Where would I find enough leather To cover the entire surface of the earth? But with leather soles beneath my feet, It’s as if the whole world has been covered.” ― Shantideva I went through the following inquiry in my twenties at a particularly low point: Maybe you think you want the whole world to change. For who? You? Those you see as victims? Some things could be better, absolutely. Hasn’t that always been the case? And how will you know when things are perfect or enough? Are you willing to put your life on hold until the world catches up with your vision of perfection? How about someone else's life? A bit risky, no? I realized that tragedy and extreme suffering will always be a part of life. This was a very sad realization but also a necessary one. I confronted the necessity to take my life and well-being into my own hands. I also had to acknowledge my zone of influence, which was and is quite small. I had to learn to take comfort that the good I do in my life and the lives around me will ripple out through time and space in ways I can’t understand. So will the bad. Sometimes we might think there is a way to “Nerf” the world. That is to say, cover the entire world in softness so that everything and everyone feels good, safe, and easy. Folks have come into my office sort of demanding or begging that life stop being so hard on them. This magical thinking usually stems from prolonged desperation and overwhelm and an externally skewed locus of control.  It’s common for mental health professionals to want easier circumstances for their clients too. It can be so hard to watch so many people go through unimaginable pain. We just want to rescue people from unjust circumstances so badly because we care so much about helping have good lives. It can feel intolerable to watch the good life be unattainable for some. The following is an allegory for why we and those we care for must struggle sometimes. I want to add a caveat that, while it is true that struggle is good for us, we must still work to advocate for marginalized people and eliminate as much unnecessary struggle as possible. Life is hard enough. We do not need racism and other prejudice in addition. The Monk and The Moth Once upon a time in a serene monastery nestled amidst lush mountains, there lived a wise and compassionate monk. The monk was known for his deep understanding of the interconnectedness of life and his ability to find beauty and lessons in every aspect of nature. One day, as the monk strolled through the monastery gardens, he came across a delicate moth struggling to emerge from its cocoon. The creature seemed trapped, its wings tangled in the fibers that once provided protection. Moved by compassion, the monk decided to help the struggling moth. With great care, he took a small pair of scissors and delicately cut away the cocoon, allowing the moth to emerge freely. As the moth unfolded its wings, the monk marveled at its beauty. However, to his surprise, the moth fluttered weakly and then fell to the ground, unable to fly.  The monk watched in sorrow as the moth struggled in vain. It soon became clear that the premature intervention had left the moth's wings and body underdeveloped and full of fluid. The struggle to break free from the cocoon was essential for the moth's wings to gain strength and for the excess fluid to be squeezed from the moth’s body.
Reflecting on the unintended consequence of his compassionate act, the monk realized that the struggle was a vital part of the moth's transformation. In trying to alleviate its immediate challenge, he had unintentionally hindered the natural process necessary for the moth's survival. As the moth's life flickered away, the monk bowed his head in remorse, understanding the profound lesson the universe had imparted through this delicate creature. He realized that sometimes, the hardships and struggles we face are intrinsic to our growth, resilience, and the development of our inner strength. The story of the monk and the moth served as a reminder within the monastery. The monk acknowledged that the intricate dance of life often requires a delicate balance between compassion and allowing the natural course of events to unfold. Closing Thoughts We have to struggle and people we care about have to struggle. Often, it is more loving and helpful to tolerate and encourage the struggle instead of trying to alleviate it. Being willing to accept and find the lessons in the struggle fosters resilience over time, covering our feet in leather in a world that will never be totally soft. Forgive me for the woefully incomplete treatment of this idea. I wanted to get this into the mix of my blog topics so I can think about how it integrates with my other ideas.
Psychotherapy, at its core, can be seen as an application of philosophy, with different therapeutic modalities embodying specific philosophical perspectives. Somatic therapy can be thought of as applied phenomenology, in particular, where we focus on experiences manifesting in the moment. The philosophy of Phenomenology is reflected in somatic therapy in that it focuses on the subjective in-the-moment appearance of phenomena to an individual. This essay explores the relationship between philosophy and empiricism in the context of somatic psychotherapy, examining how these seemingly divergent approaches coalesce to create synergistic results. Philosophy in Somatic Therapy: Somatic therapy, which reflects the philosophy of phenomenology, partially operates on the premise that experiences emerge spontaneously in the present moment. Much like phenomena appearing in real life in phenomenology, somatic therapy delves into the immediacy of bodily sensations, movements, and experiences. This emphasis on the subjective, lived experience aligns with the phenomenological exploration of consciousness and the essence of experience. In other words, in somatic therapy, we avoid trying to interpret a topic of interest and instead focus on recreating the elements of it that we can in the room (i.e. through the use of projective objects and observing the body along with the emergent elements in the mind like spontaneous images). Antithesis of Empiricism: The immediacy of experiences in somatic therapy is antithetical to empiricism, which emphasizes observable "evidence" that there is a consistent "truth" across contexts that we can obtain through systematic evaluation, that is, the scientific method. While empiricism seeks tangible and measurable outcomes, phenomenology, particularly in the somatic context, values the subjective and spontaneous nature of human experience that invites the meaning-making of the person who experiences it. This inherent tension has historical roots, with empiricism initially appearing to be at odds with phenomenological and somatic approaches in turn. Synergy in Somatic Therapy: Despite the apparent dichotomy, modern somatic therapy demonstrates a unique synergy between phenomenology and empiricism, a combination that can be described as "toward" pragmatism as outlined in this beautiful essay by O.G. Rose. In a somatic therapy session, the subjective immediacy of phenomenological experiences is harnessed, providing a rich landscape for exploration. Empiricism, with its systematic evaluation, then complements this process by validating and verifying the generalized efficacy of somatic interventions. Furthermore, traditional evidence-based approaches bolster the efficacy of somatic therapeutic processes by acting as a measuring tool for how well someone is progressing in therapy as well as contributing valuable psychoeducation that orients the client. Together, they contribute to a holistic understanding of the human experience. For example, concepts like ‘formerly helpful belief systems that are no longer adaptive and cause problems for clients’ are core tenets of cognitive therapists. In the paraphrased words of one of my Sensorimotor Psychotherapy Trainers “cognitive therapies are necessary but not sufficient for genuine psychological transformation.” A client may know that they have faulty thinking but a part of them still holds that outmoded belief, along with its emotions and behaviors. Thus, when somatic therapy supports that part in transforming, we will have accomplished the goal that cognitive therapy sets out to do but is unable to provide in certain cases with its current set of tools and approaches. We need cognitive therapy’s goals and objectives so that we know we are on the right track with the somatic therapy. When both clients and counselors alike know what we want to accomplish and why, we are empowered by having direction and clarity and held accountable by grounded, empirically demonstrated measurements. Evolution of Empiricism's Perspective: Historically, evidence-based practices have been skeptical of working with the type of emergent material that somatic practices embrace. Emergent parts, memories, emotions, and the expression of these in the body were treated as things about which to educate the client, provide a cognitive framework to apply to oneself, and simply see how one’s logic is faulty, which was thought to be enough to provide a behavior change. However, certain enclaves of empirical researchers, like the presenters at the Interpersonal Neurobiology Conference, have shifted their stance over time, recognizing the value of phenomenological approaches in somatic therapy, primarily because we now have much better frameworks for understanding how psychological injury, a.k.a. trauma, functions in the nervous system. The integration of these perspectives has broadened the therapeutic landscape, allowing for a more nuanced understanding of the mind-body connection. Phenomenology Ahead of Empiricism: Within the somatic and other fields of study, phenomenology often outpaces empiricism in capturing the intricacies of human experience. In the study of the history of science, it is evident that experiments are inspired by how life appears to researchers. For example, Newton observed the apple falling and was inspired to create thought experiments that lead to the invention of calculus. He says in his letter to a friend named William Stukeley: "...the notion of gravitation came into my mind. All of a sudden, the apple, as far as I can make out, left the tree. Why should that apple always descend perpendicularly to the ground, thought I to myself. Why should it not go sideways, or upwards? But constantly to the earth’s surface... the reason is, that the earth draws it. There must be a drawing power in matter." The immediacy and subjectivity of somatic practices, such as emotions expressed in the body or images that appear in the mind eye, provide individuals with profound insights into their embodied existence. The manner in which these transformative insights are gained by means of somatic approaches has preceded and is in some instances still ahead of empirical validation, showcasing the unique ability of phenomenology to explore uncharted territories of the mind-body connection and other aspects of life. Of course, there is a long history as well that our interpretation of phenomena leads us astray. Therefore the eternal dance of phenomenological exploration and empirical validation is necessary for us to continue to approach “Truth…” or something like that. Challenges and Growth: While somatic therapy being ahead-of-its-time creates challenges in the field insofar as many of our approaches have yet to be empirically validated, it also prompts growth and innovation. Pioneering somatic therapists continue to explore new techniques and approaches rooted in phenomenological principles, pushing the boundaries of empirical research. This dynamic relationship fosters an evolving and responsive field that prioritizes the immediate needs and experiences of clients. In conclusion, the interplay between philosophy and empiricism in somatic psychotherapy reflects the dynamic tension between the immediacy of phenomenological experiences and the systematic evaluation of empiricism. Somatic therapy, as applied phenomenology, attempts to capture the essence of human existence in the moment, challenging the conventional boundaries of evidence-based practices. The evolving relationship between these two perspectives highlights the importance of embracing both the immediacy of experience and the empirical validation in the pursuit of a comprehensive and effective therapeutic model. |
AuthorProsopon Therapy Archives
July 2024
Categories |
||||
 RSS Feed
RSS Feed