|
From my perspective, a cognitive distortion arises when a “part” or subpersonality is activated and in distress. A Part is any subpersonality that arises that is not the “compassionate witnessing observer” (CWO). People sometimes refer to their “parts” as sides, modes, etc. of themselves (“I have a dark/wild/naive/youthful/serious side,” “I can really get into hyperfocus mode,” “part of me just loves to dance and I have to take him out to the honky-tonk,” etc.)
The “compassionate witnessing observer” (CWO) is called many things by many spiritual and therapeutic traditions. This is what I choose to call it. Qualities of the CWO include, objectivity, seeing the “good” in everything and everyone but also recognizing when a “good” being is not acting in the best interest of itself or others usually because of confusion. The CWO feels settled and self-assured, calm patience, wholeness, comfort with awareness and presence, and more. When a part is present it does not necessarily mean that the part is in distress. When someone feels distress, however, a part is always present and contains the distress. This is ok, expected, and particularly functional when the part is also connected to the CWO. When the part is not connected to the CWO, is when larger problems can occur. Whether or not the part is connected to the CWO, if the part is in distress, it is likely that the part is embodying a cognitive distortion. A cognitive distortion is when someone's thinking does not align with reality and what someone can reasonably know about reality. Each distortion arises in response to a body state that emerged as a reactive adaptation to the environment and produces a responding body state that further attempts to adapt usually to a suboptimal situation. All body state responses are unique to the individual. As you read through these, notice what your body does. Stick with sensation (tingly, hot, metallic, collapsed, watery, foggy, etc.) rather than story or emotional words. Do your best to stay in touch with your CWO. If you have not had a direct experience with your CWO, that’s ok. However, you are more likely to become triggered, defensive, activated, or have some kind of difficulty in general as you read and feel through this list. Stop the exercise if you reach a limit. All-or-Nothing Thinking (Black-and-White Thinking): Seeing situations in extremes, without recognizing middle ground or shades of gray. Overgeneralization: Drawing broad conclusions based on limited evidence, often making predictions about future events based on a single negative experience. Filtering (Selective Abstraction): Focusing exclusively on the negative aspects of a situation while ignoring any positive elements. Jumping to Conclusions:
Personalization: Blaming oneself for external events or circumstances beyond one's control, or attributing external events to personal actions when there is no evidence for such a connection. Should Statements: Setting rigid and unrealistic standards for oneself or others and feeling guilty or upset when these standards are not met. Labeling and Mislabeling: Assigning global, negative labels to oneself or others based on errors or mistakes, rather than recognizing the specific behavior. Emotional Reasoning: Assuming that because one feels a certain way, the feelings must be accurate reflections of reality. Discounting the Positive: Minimizing or dismissing positive experiences, qualities, or accomplishments, often attributing them to luck rather than personal effort. Mind Bluffing: Believing negative thoughts without questioning their validity, taking them at face value. Control Fallacies:
You made it to the bottom of the list! Take a movement, breathing, water, or presence break. Come back to center. Reconnect to your CWO. What did you learn about yourself?
0 Comments
2/18/2024 Object Relations Theory: A Classical Conceptual Foundation for Understanding Modern Attachment TheoryRead NowI am adding a discussion of Object Relations Theory to my blog because it is a theory that has greatly influenced my work. In my opinion it is the beginning of the discussion of attachment and still provides a worthwhile perspective to the modern clinician or informed client despite being a classical theory.
At the end of this article I lay out Mahler’s stages of separation in early life. I do this because the nature of the primary wounding in the client can often be located within one of these stages. Knowing at what stage the client is wounded is useful because the way I as the therapist behaves toward the client is different depending on the wound stage. Object Relations Theory is a psychoanalytic theory that focuses on the way individuals relate to others, particularly in the context of interpersonal relationships. Developed within the psychoanalytic tradition, this theory departs from Freudian drive theory, emphasizing the importance of interpersonal experiences and relationships in shaping an individual's psychological development. The term "object" in Object Relations Theory does not refer to inanimate objects but rather to significant people (objects) with whom an individual interacts, such as parents, caregivers, or other important figures. The theory suggests that early relationships, especially with primary caregivers, play a crucial role in the formation of an individual's mental representations or "internal objects." Key concepts in Object Relations Theory include: Internal Objects: Mental representations of others that influence how individuals perceive and interact with people in their lives. These internal objects are shaped by early caregiving experiences. Attachment: Object Relations Theory is closely related to attachment theory, emphasizing the impact of early attachment experiences on emotional and relational development. Transference and Countertransference: These concepts involve the projection of feelings and expectations onto others (transference) and the emotional reactions of the therapist (countertransference) in a therapeutic relationship. Splitting: The tendency to perceive people or situations as all good or all bad, reflecting a lack of integration of positive and negative qualities in others. Introjection: The process of internalizing external objects, incorporating aspects of others into one's own sense of self. Object Relations Theory has been influential in the field of psychotherapy, especially in psychodynamic and relational approaches. Therapists utilizing this perspective aim to explore and understand how past relationships and internalized objects impact a person's current emotional and relational functioning. Here is a list of some key figures associated with Object Relations Theory and the nature of their contributions: Melanie Klein: A pioneering psychoanalyst who made significant contributions to Object Relations Theory. She focused on the early stages of infant development and the impact of internalized objects on psychological functioning. Anna Freud: Continued her father’s work by emphasizing the impact of early childhood experiences, particularly the mother-infant relationship, on the formation of internalized mental representations and object relations in individuals Donald Winnicott: Known for his work on object relations, transitional objects, and the "good enough mother" concept. Winnicott emphasized the importance of the mother-infant relationship in shaping the individual's sense of self. Ronald Fairbairn: Contributed to the development of Object Relations Theory, emphasizing the role of internalized objects and the impact of early relationships on personality development. Wilfred Bion: Extended Object Relations Theory by introducing concepts like "container-contained" and "alpha function." Bion explored the emotional and cognitive aspects of the mother-infant relationship. Margaret Mahler: Known for her research on infant development and separation-individuation processes. Her work has been influential in understanding the early formation of object relations. Harry Stack Sullivan: While not exclusively an Object Relations theorist, Sullivan's interpersonal theory influenced later developments in Object Relations Theory. He emphasized the role of interpersonal relationships in shaping personality. Otto Kernberg: Integrated Object Relations Theory with psychoanalytic concepts and made contributions to understanding personality disorders, particularly focusing on borderline personality organization. Heinz Kohut: Developed Self Psychology, a branch of Object Relations Theory, focusing on the role of self-objects and the formation of a cohesive sense of self. D.W. Winnicott: A psychoanalyst who extended Winnicott's ideas and made further contributions to Object Relations Theory, particularly in the areas of play and creativity. Margaret Mahler, a psychoanalyst and researcher, proposed a developmental model known as the Separation-Individuation theory within the context of Object Relations. This theory outlines stages in the early development of infants as they form a sense of self and relatedness to others. The key stages in Margaret Mahler's Separation-Individuation theory are:
Margaret Mahler's stages of development emphasize the gradual process of separation and individuation, with a focus on the evolving relationship between the infant and the primary caregiver. If there is a major disruption at one or more of these stages, the likelihood of maladaptation increases and shows up in a manner that is associated with the stage at which the disruption occurred. This is useful to know as a clinician or client because the solution to the wound can be found in the task of the stage at which the wound occurred. This notion that the wound contains the antidote is common across psychological theories and, in my experience, pans out in the actual practice of psychotherapy.
What is Past Reality Integration (PRI)?
PRI, created by Ingeborg Bosch, operates on the assumption that emotions and behavioral patterns impacting our daily lives are rooted in old traumas from our early years, often unbeknownst to us. Whether grappling with depression, burnout, anxiety, panic attacks, addiction, eating issues, or relationship challenges, PRI posits that the origin of these problems lies in past experiences, veiling the residual pain from that time. In PRI therapy, your therapist guides you to apply PRI techniques independently based on your specific concerns, a process established during an intake interview. Through careful observation and utilization of the PRI model, which elucidates the workings of the brain, you gain deeper insights into your emotions and defenses. The therapeutic process involves consciously halting habitual behaviors to access latent, unconscious feelings linked to your past. The ultimate goal is not to perpetuate the experience of old pain but to progressively live without unnecessary challenges and defenses. PRI therapy enables you to swiftly recognize and dismantle activating behaviors, allowing you to experience the present unburdened and fostering authentic connections with yourself and your environment. The Handout The handout available for download at the top of this webpage lists off the defenses people commonly use to protect against perceptions of abandonment, rejection, and neglect. On the first page, you'll see each defense listed and the antidote to it right after. Below the defense-antidote you will see the "narrative" of the defense or the thoughts that go with it. On the second page, you will see the PRI model of a trigger. At the bottom of the second page you see on the left the trigger getting integrated and on the right the trigger getting suppressed and filed back into the unconscious. A defense mechanism is a subconscious psychological strategy employed by individuals to cope with and manage emotions, particularly anxiety or stress, by protecting themselves from thoughts, feelings, or impulses perceived as threatening or distressing. These mechanisms operate outside of conscious awareness and are aimed at maintaining psychological balance and protecting self-esteem. Introduced by Sigmund Freud and further developed by other psychologists, defense mechanisms include many different processes, including the ones listed below. While these mechanisms can be adaptive in moderating emotional distress, their overuse or misuse may lead to maladaptive coping strategies, hindering personal growth and well-being.
Repression: Unconsciously forgetting or blocking out unpleasant memories or thoughts. Denial: Refusing to acknowledge the existence of something distressing or threatening. Projection: Attributing one's own unacceptable thoughts, feelings, or motives to others. Displacement: Redirecting emotions or impulses from their original source to a less threatening one. Sublimation: Transforming socially unacceptable impulses or urges into socially acceptable actions. Rationalization: Offering logical or reasonable explanations for behaviors or thoughts that are actually driven by irrational motives. Regression: Reverting to an earlier stage of psychological development in response to stress or conflict. Reaction Formation: Expressing the opposite of what one truly feels or thinks, often as a defense against unacceptable impulses. Intellectualization: Dealing with emotional conflicts or stress by focusing on abstract or intellectual aspects. Suppression: Consciously choosing to not think about or dwell on certain thoughts or feelings. Undoing: Engaging in behavior to counteract or "undo" guilt or anxiety resulting from unacceptable thoughts or actions. Identification: Associating oneself with someone or something in order to enhance self-esteem or reduce anxiety. Fantasy: Creating an imaginary world to escape from or compensate for perceived deficiencies in reality. Compensation: Overachieving in one area to make up for perceived failures or shortcomings in another. Splitting: Viewing people, situations, or oneself in extremes of either all good or all bad, to avoid the anxiety of ambivalence. Somatization: Expressing emotional distress through physical symptoms or ailments. Acting Out: Engaging in impulsive or inappropriate behavior as a way of expressing unconscious emotions. Humor: Using humor as a defense mechanism to cope with distressing situations or emotions. Sour Grapes: a cognitive strategy in which individuals, unable to attain something they desire, devalue or dismiss the desired object or goal as unimportant or undesirable to ease the emotional impact of unmet needs. Selective Forgetting: "Choosing" to remember only certain details of an event while forgetting others to protect oneself from discomfort. Isolation of Affect: Separating feelings from ideas and events, dealing with emotional aspects in a detached and intellectualized manner. Compartmentalization: Separating conflicting thoughts or emotions into separate compartments to avoid internal conflict. Minimization: Downplaying the significance of one's thoughts, feelings, or actions to reduce anxiety or guilt. Idealization: Seeing someone or something as perfect, admirable, or superior as a way to avoid dealing with negative feelings. Withdrawal: Physically or emotionally removing oneself from a situation to avoid potential stress or conflict. Passive-Aggression: Indirectly expressing hostility or anger through passive means rather than directly confronting the source. Sarcasm: Using humor or irony to mock or convey contempt in a way that masks true feelings. Autistic Fantasy: Retreating into a rich fantasy life to escape from reality and cope with emotional stress. Projective Identification: Projecting positive or negative thoughts or feelings onto another person and simultaneously reacting with the projected material as if it now belongs to the other person. Self-Serving Bias: Attributing positive events or successes to one's own character while attributing negative events or failures to external factors. Spiritual Bypassing: Using spiritual beliefs or practices to avoid dealing with unresolved psychological issues. Compulsive Behavior: Engaging in repetitive, ritualistic actions to alleviate anxiety or prevent a feared event from occurring. 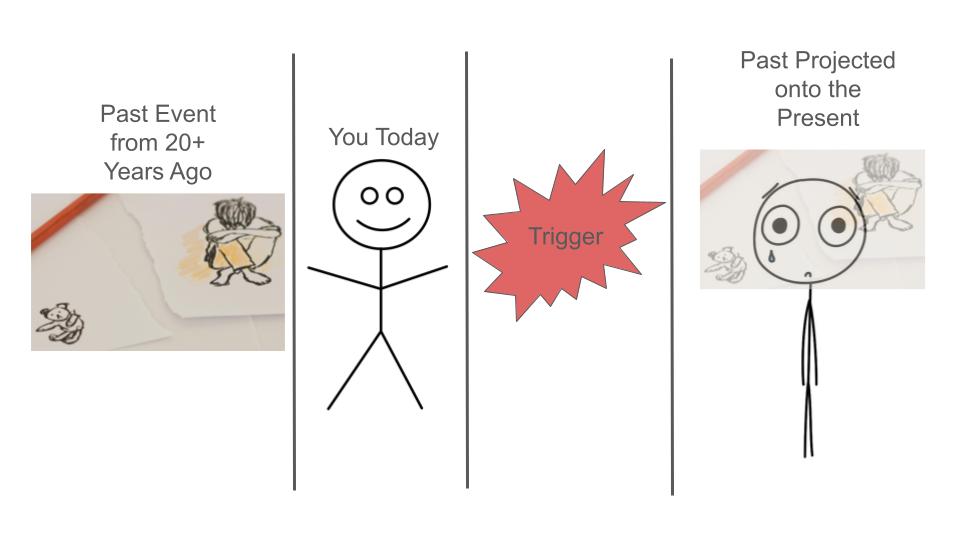 How does getting "triggered" work?
Trigger Logic: this refers to the the thought pattern related to maintaining the intensity and "flavor" of the trigger. When in the process of a trigger, we can feel like it is of the utmost importance to maintain the triggered state; that to let it go would compromise our integrity, safety, or goal in the moment. The thoughts can say to us that it is impossible to regulate. To even think of regulating can feel threatening, insulting, or shaming. It Just Feels So Real: The reason its hard to "reason" with a trigger is because your body really feels like its in the original past event while your mind does not have the sensation of remembering. So you are actually feeling the past but absolutely cannot distinguish it from the present. In our example, the loss of the keychain object feels like the forced removal of the stuffed animal when you were a little child. The self attack you engage in is the defense you used as a child to deal with the wound created by the misattuned parent. When the stuffed animal was taken away, your little body went into chaos. You didn't understand what was happening and blamed yourself, because that is what little children do to maintain the notion that their caregivers are "good, reliable, and worthy of trust." It is safer for a child to think that they are the problem rather than the adults because they rely on the adults for survival. So, when you are triggered, you essentially "forget" you are an adult and feel like a threatened child, teenager, or some other past disempowered version of yourself. You experience that past version in your body and you feel like that version is you in the here and now, even though it is not, in fact, you currently. Regulation: Its Not So Easy. Just because there is a thought component to trigger logic does not mean that it is easy to "just regulate" in the moment. Regulating take a ton of awareness and practice. People who have been able to practice genuine regulation are lucky, privileged, and hard-working because genuine regulation practices are hard to come by and, at times, hard to learn. Once someone understands how to regulate and their particular needs regarding regulating, the process can become quite simple. The road to simplicity can be a long and harrowing one, however, with many opportunities for illusions, mysteries, and traps along the way. How do I learn to regulate?
How do I know that I am regulating and not dissociating or coping with compartmentalization? In essence, you will be able to assess the objective magnitude of an event in terms of its level of threat towards you and others. You will be able to recognize that most unpleasant events are uncomfortable and inconvenient but are not emergencies or a sign that either you or the world are completely awful. Your emotions will serve as trustworthy messengers rather than threatening energies that totally overwhelm you. You will be able to think and feel at the same time and be able to choose a course of action that is in your and other's best interest. Survivor Bias
I wanted to address survivor bias because I often talk about how to achieve positive outcomes in mind-body health care. I felt it would be unethical not to mention the reality that not everyone heals. It is so tempting to stay focused on those who heal and how they did it, but ultimately, it can be really hard to discern what caused the healing, especially because I tend to advocate that my clients pursue a multidisciplinary route to healing. Privilege It should also be noted that there is a lot of privilege at times in being able to pursue a multipronged healing approach. I personally sit with grief that transformation is not available to all who desire it. Here are some of the way that survivor bias interferes with our ability to better understand the crux of healing in both mainstream and alternative healthcare: Survivor Bias in Mainstream Healthcare Survivor bias in health outcomes refers to the distortion that can occur when analyzing data or drawing conclusions about health based only on individuals who have survived or reached a certain point in a study, treatment, or condition. This bias arises when individuals who did not survive or dropped out of the study are not included in the analysis, leading to an incomplete and potentially misleading understanding of health outcomes. Here are a few examples to illustrate survivor bias in health outcomes: Clinical Trials: If a clinical trial only reports the outcomes of participants who completed the study and ignores those who dropped out due to adverse effects or lack of improvement, there may be a biased representation of the treatment's effectiveness. Including only "survivors" in the analysis can overstate the positive effects and underestimate potential risks. Longitudinal Studies: In studies tracking the health outcomes of a particular population over time, survivor bias can occur if the analysis is based solely on individuals who have reached a certain age or milestone. This may lead to an overly optimistic view of the population's health, as those who experienced negative health outcomes or premature death are not considered. Disease Registries: When compiling data from disease registries or databases, survivor bias can occur if only individuals who are still alive or actively seeking treatment are included. This might lead to an underestimation of the severity of the disease or the effectiveness of certain treatments. Observational Studies: In observational studies where individuals self-select into treatment groups, survivor bias may occur if only those who respond positively to a particular intervention continue to participate or report their outcomes. This could create a falsely positive impression of the intervention's efficacy. To address survivor bias in health outcomes, researchers need to consider the entire population under study, including those who did not survive or dropped out. Analyzing complete datasets allows for a more accurate assessment of the factors influencing health outcomes and helps avoid drawing conclusions based solely on individuals who have "survived" a particular point in the process. Survivor bias in Alternative Health Care: Survivor bias can also be relevant when evaluating health outcomes in the context of alternative healthcare practices. In this context, survivor bias may manifest in various ways, potentially affecting the perception of the efficacy and safety of alternative treatments. Here are a few scenarios where survivor bias might be observed in alternative healthcare: Self-Selection Bias in Testimonials: Individuals who have positive experiences with alternative healthcare treatments may be more inclined to share their success stories or testimonials. This self-selection bias can create an unrepresentative sample, as those who did not experience positive outcomes or had negative reactions may be less likely to report their experiences. Online Communities and Forums: Discussions in online health forums or communities may primarily involve individuals who have had positive experiences with alternative treatments. Negative experiences or lack of efficacy might be underrepresented, leading to a skewed perception of the success rates of these treatments. Long-Term Follow-Up: Alternative healthcare practices often lack rigorous long-term studies and follow-up assessments. If individuals who initially report positive outcomes are followed up, while those who did not experience benefits or faced adverse effects drop out of follow-up studies, survivor bias may lead to an overestimation of treatment success. Exclusion of Unsuccessful Cases in Research: Some alternative healthcare studies may selectively report positive results and exclude cases where the treatment did not work or caused harm. This can lead to an inflated perception of the overall success of the treatment. Underreporting of Adverse Events: Individuals who have adverse reactions to alternative healthcare treatments may be less likely to report these events, especially if the treatment is perceived as unconventional or not widely accepted in mainstream medicine. This can result in an incomplete understanding of the potential risks associated with alternative therapies. To mitigate survivor bias in alternative healthcare, it's essential to approach the evaluation of treatments with a critical and evidence-based perspective. Researchers and practitioners should strive to collect comprehensive data, including both positive and negative outcomes, and conduct well-designed studies that account for potential biases. Additionally, individuals seeking alternative healthcare should be aware of the importance of reporting both positive and negative experiences to contribute to a more balanced understanding of the treatments they explore. Humility and Balance In acknowledging the reality of survivor bias, it's crucial to foster a compassionate and honest dialogue about the complexities of healing in both mainstream and alternative healthcare. While we often share success stories and pathways to positive outcomes, it's equally important to recognize that not everyone's journey leads to healing. This acknowledgment doesn't diminish the value of those who find transformation but instead invites us to approach discussions with humility and empathy. Healing is multifaceted, and the pursuit of well-being is often influenced by various factors, including access to resources and personal circumstances. As we delve into the challenges posed by survivor bias, we're presented with an opportunity for growth and a commitment to understanding health outcomes more comprehensively. By encouraging a transparent and inclusive approach in research, we can navigate the complexities of both mainstream and alternative healthcare, ensuring that the experiences of all individuals, regardless of their outcomes, contribute to a more nuanced and balanced understanding of health and healing. Challenges in Implementing Change
I’ve worked with some really challenging psyches, especially my own. I’ve seen mind boggling transformations. I’ve also seen people languish for years in the doldrums or agony while wondering why transformation seems out of reach for this person and not for another. The interventions we offer are hugely important in creating the change, but if the seed of change is planted on unprepared soil, very little or nothing is likely to grow. The person receiving the intervention must know already or learn how to accept change once it has been made. This is a necessary condition that is often overlooked by professionals when prescribing special diets, meditation plans, and even surgeries and medicine. If a client does not know how to change and be different, I believe the likelihood of an intervention working is impacted. Upper Limits Problem This is something akin to the upper limits problem. The "upper limits problem" refers to a psychological phenomenon where individuals set self-imposed ceilings on their achievements or capabilities, often without realizing it. People may unknowingly sabotage their own potential by subconsciously adhering to these limits, which can hinder their progress and prevent them from reaching their full potential. Overcoming the upper limits problem requires self-awareness, introspection, and a willingness to challenge ingrained beliefs and behaviors in order to break through these artificial barriers and unleash one's true capabilities. The willingness necessary to change may be hard won, however, depending on how dysregulated a person’s nervous system is. The Resourcing Phase This is why the “resourcing” phase is so crucial. The resourcing phase in trauma therapy means training the nervous system to be regulated enough for trauma processing. That does not mean “applying” regulation techniques like breathing, positive thinking, stretching and so on. Rather that means validating pain in the client in a specific way that enables the resources to emerge on their own. Due to the non-linear nature of this process and the varieties of nervous system presentations, this phase can take a long time or be the only phase that a client ever works on. I really want to believe that nervous system healing is possible for everyone, barring extreme damage to the system. I hope that as we continue to learn more about the nervous system that we get increasingly better and efficient at helping people make lasting changes despite innate challenges. Cognitive Dissonance and Belief Systems This week in my practice I became more aware of how cognitive dissonance presents in clients who seem to experience better psychological states and then fall back into old patterns and systems of belief over and over again. It is so important to note that “just changing your belief system” is not a thing. Occasionally we see a radical change in belief system but instances such as these are outliers and not the norm. Beliefs are embodied and the embodied experience of a belief must change along with the “words in the head” (thoughts). Typically I see progress being made in clients like an inchworm, to put it in an overly simplistic way. Half of them get to a new state then the other half catches up and on and on. Cognitive dissonance is a psychological theory developed by Leon Festinger in 1957. It refers to the discomfort or mental tension that a person experiences when they hold two or more conflicting beliefs, attitudes, or values simultaneously, or when their behavior conflicts with their beliefs or values. The key idea behind cognitive dissonance is that individuals strive for internal consistency in their thoughts, beliefs, and attitudes. When inconsistencies arise, they are motivated to reduce the discomfort by changing one of the conflicting elements. This can happen through various means, such as changing one's beliefs, acquiring new information to support existing beliefs, or minimizing the importance of the conflict. For example, if someone is aware that smoking is harmful to health but continues to smoke, they may experience cognitive dissonance. To reduce this discomfort, they might downplay the risks of smoking, convince themselves that they have other healthy habits, or find other ways to justify their behavior. Cognitive dissonance theory has been widely used to explain various psychological phenomena, including attitude change, decision-making, and rationalization of behavior. Addressing Cognitive Dissonance Addressing cognitive dissonance involves acknowledging and resolving the conflicting beliefs, attitudes, or behaviors causing discomfort. Here are some strategies to directly address cognitive dissonance: Awareness: to become aware of the cognitive dissonance is half the battle. Furthermore, acknowledging and admitting that one is in a cognitive dissonance dynamic invites intentionality rather than reactivity when it comes to addressing the dissonance. Somatic Exploration of Beliefs: this goes along with awareness. Beliefs are not just in the thoughts. Beliefs express through the body. If I believe that I am bad, I may have a collapsed posture. If I believe that I am worthy of love, my body may take a relaxed attitude. Seek Information: I may need to learn more about each conflicting side of the dissonance. In this context, I may need to learn more about the origin of the limiting belief in my life. In turn, I may also need to learn more about the more helpful mindset before my intellect feels comfortable with going through the change process. Explore the Golden Shadow: unhelpful beliefs are often in “parts” or subpersonalities that we have disowned. The best course of action in dealing with parts is to acknowledge that the now unhelpful belief was actually beneficial at one time and brought many gifts with it. You can then invite the part to transform and take on a new “job,” thereby more fully expressing its innate gifts. Case Example: Sonia's Struggle with Self-Worth and Self-Care Sonia, a 40-year-old executive, sought therapy to address persistent feelings of low self-worth. Despite her professional success, she struggled with a deep-seated belief that she was not worthy of care and attention, leading to challenges in implementing a self-care routine. Making time for herself brought up an unbearable feeling of friction and a panic like feeling in her body. Background: Sonia's childhood was marked by high expectations from her parents, conditioning her to believe that her value was contingent on achievement. This belief persisted into her adult life, impacting her relationships and, most notably, her ability to prioritize self-care. Presenting Issues: In therapy, Sonia expressed feeling overwhelmed by work demands and the constant need to prove herself. Despite recognizing the importance of self-care, she found it challenging to implement and sustain a routine due to an underlying belief that taking time for herself was undeserved. Pressure was mounting for her to resolve this conflict because she was beginning to develop significant digestive issues that were interfering with her ability to function. Therapeutic Process: Awareness Stage: Sonia, with the support of her therapist, became aware of the cognitive dissonance between her acknowledgment of the importance of self-care and her ingrained, felt-sense belief that she didn't deserve it. This dissonance triggered anxiety and guilt whenever she attempted self-care activities. Somatic Exploration of Beliefs: Through therapeutic conversations, Sonia explored the origins of her belief system and how that was showing-up in her body. She discovered that her worth had become tied to external validation, and any focus on self-care stirred feelings of guilt and impending inadequacy. When engaging in self-care shoe could not relax her body and take in the nourishing effects of self-care. Seeking Information: Sonia engaged in educational sessions with her therapist to understand the psychological and physiological benefits of self-care. Sonia values scientific data, so her therapist provided articles that satisfied Sonia’s intellect. This information highlighted how her negative beliefs about self-worth came from her attempts to survive her past relationship with her parents and did not make sense as a useful mode of function in her life now. Cognitive Dissonance Challenge and The Golden Shadow: Sonia faced the challenge of actively challenging her belief system. As she started incorporating small self-care practices, such as walks in nature and setting time boundaries at work, she experienced internal resistance in the form of feelings of guilt and anxiety. Sonia practiced staying with the physical sensations of her resistance as she took steps to care for herself anyway. Sonia was able to validate how useful the adaptation of self-denial was early on in her life and discovered that this “part” that self denies holds her intuitive awareness of her want and needs and how to flow through her life addressing those wants and needs while also staying on top of responsibilities and goals. Resolution and Integration: Over time, Sonia worked on reframing and reembodying her beliefs about self-worth. She discovered that her down time and boundaries not only did not detract from her value, rather, they enhanced her ability to be efficient and creative at work. Furthermore, the backlash she expected from colleagues never came and Sonia realized that people around her approved of her prioritizing herself. The therapist guided her in developing a self-compassionate narrative and understanding that self-care was not only deserved but crucial for her overall well-being and, secondarily, her performance as a worker. Outcome: As Sonia persistently confronted her cognitive dissonance, she began to see positive changes. The implementation of a self-care routine, initially met with inner conflict, became more natural. Sonia reported feeling more in flow, resilient to work stress, and, most importantly, a growing sense of embodied self-worth detached from external achievements. Closing thoughts: This case highlights the intricate relationship between self-worth and the ability to prioritize self-care. Through somatic exploration, embodied parts work, gentle exposure therapy, Sonia experienced organic cognitive restructuring and successfully navigated the cognitive dissonance, fostering positive changes in her beliefs and daily practices. You can see why it is hard for individuals to make big changes at times. An important stage of change I am noticing in my own processing is the need to intentionally create integration time after a big session. It goes like this: I work on a big wound, the session ends on a note of care, love, and self-compassion, and then I am facing the unknown. My personality now has the opportunity to update, but I must make space for the unknown. There is a tendency for humans to fill in the unknown with old stories, interpretations, and explanations. For my personality to really update, I have to know what the unknown feels like and intentionally stay there for awhile with curiosity about what will come through next. I allow my personality to update spontaneously rather than imposing an ideal created by my thoughts. In this way, I consciously confront the upper limits problem and cognitive dissonance to that the new can emerge. If you are new to the mental health treatment world, you may feel confused and overwhelmed by the different letters at the end of practitioners names. Here is a glossary of mental health practitioner types and licenses.
Psychiatrist: A medical doctor (MD) or doctor of osteopathic medicine (DO) specializing in the diagnosis, treatment, and prevention of mental illnesses. Psychiatrists can prescribe medication. Psychologist: A professional with a doctoral degree (Ph.D. or Psy.D.) in psychology, trained to diagnose and treat mental health disorders through therapy and counseling. Licensed Professional Counselor (LPC): A mental health professional with a master’s degree in counseling or a related field. LPCs provide therapy and counseling services to individuals, couples, and families. Clinical Social Worker (LCSW): A licensed social worker with a master’s degree in social work and specialized training in clinical practice. LCSWs offer therapy, counseling, and support services. Marriage and Family Therapist (LMFT): A mental health professional with a master’s or doctoral degree in marriage and family therapy. LMFTs specialize in working with couples and families to address relationship issues. Psychotherapist: A generic term for professionals who provide talk therapy to address emotional and psychological issues. This term can encompass psychologists, social workers, counselors, and psychiatrists. Psychiatric Nurse Practitioner (PMHNP): A nurse practitioner with specialized training in psychiatry. PMHNPs can assess, diagnose, and treat mental health disorders, including prescribing medication. Substance Abuse Counselor/Licensed Addiction Counselor (LAC): A professional trained to help individuals struggling with substance abuse and addiction. They may hold various degrees, including LPC, LCSW, or specific certifications. Supervisor: A counseling supervisor is an experienced and credentialed professional who provides guidance, oversight, and support to counselors-in-training or practicing counselors to enhance their clinical skills, ethical conduct, and professional development. Milieu Therapist: A therapist who works within a therapeutic environment or community setting, actively shaping the therapeutic milieu to facilitate positive social interactions and promote the well-being of individuals receiving mental health services. Group Counselor: A professional who facilitates therapeutic sessions with a group of individuals, fostering mutual support, communication, and personal growth within the group dynamic. Couples Counselor: A professional who specializes in providing therapy and guidance to couples, assisting them in resolving conflicts, improving communication, and enhancing their relationship. Case Worker: A professional who assesses, plans, coordinates, and advocates for the services and resources needed by individuals or families to address their specific needs and improve their overall well-being. Sex Therapist (CST): a specialized mental health professional who helps individuals and couples address and navigate issues related to sexuality, intimacy, and sexual health through counseling and therapeutic interventions. Sex Addiction Therapist (CSAT): a mental health professional who specializes in assisting individuals with compulsive sexual behaviors, employing therapeutic interventions to address and manage issues related to sex addiction. Art Therapist: A mental health professional who uses art-based interventions to help individuals explore and express their emotions. Art therapists may have degrees in art therapy or related fields. Music Therapist: A therapist who uses music-based interventions to address emotional, social, and cognitive issues. Music therapists may have degrees in music therapy or related fields. Behavior Analyst: A professional trained in applied behavior analysis (ABA) to assess and address behavioral issues, often working with individuals with autism spectrum disorder or developmental disabilities. “Where would I find enough leather To cover the entire surface of the earth? But with leather soles beneath my feet, It’s as if the whole world has been covered.” ― Shantideva I went through the following inquiry in my twenties at a particularly low point: Maybe you think you want the whole world to change. For who? You? Those you see as victims? Some things could be better, absolutely. Hasn’t that always been the case? And how will you know when things are perfect or enough? Are you willing to put your life on hold until the world catches up with your vision of perfection? How about someone else's life? A bit risky, no? I realized that tragedy and extreme suffering will always be a part of life. This was a very sad realization but also a necessary one. I confronted the necessity to take my life and well-being into my own hands. I also had to acknowledge my zone of influence, which was and is quite small. I had to learn to take comfort that the good I do in my life and the lives around me will ripple out through time and space in ways I can’t understand. So will the bad. Sometimes we might think there is a way to “Nerf” the world. That is to say, cover the entire world in softness so that everything and everyone feels good, safe, and easy. Folks have come into my office sort of demanding or begging that life stop being so hard on them. This magical thinking usually stems from prolonged desperation and overwhelm and an externally skewed locus of control.  It’s common for mental health professionals to want easier circumstances for their clients too. It can be so hard to watch so many people go through unimaginable pain. We just want to rescue people from unjust circumstances so badly because we care so much about helping have good lives. It can feel intolerable to watch the good life be unattainable for some. The following is an allegory for why we and those we care for must struggle sometimes. I want to add a caveat that, while it is true that struggle is good for us, we must still work to advocate for marginalized people and eliminate as much unnecessary struggle as possible. Life is hard enough. We do not need racism and other prejudice in addition. The Monk and The Moth Once upon a time in a serene monastery nestled amidst lush mountains, there lived a wise and compassionate monk. The monk was known for his deep understanding of the interconnectedness of life and his ability to find beauty and lessons in every aspect of nature. One day, as the monk strolled through the monastery gardens, he came across a delicate moth struggling to emerge from its cocoon. The creature seemed trapped, its wings tangled in the fibers that once provided protection. Moved by compassion, the monk decided to help the struggling moth. With great care, he took a small pair of scissors and delicately cut away the cocoon, allowing the moth to emerge freely. As the moth unfolded its wings, the monk marveled at its beauty. However, to his surprise, the moth fluttered weakly and then fell to the ground, unable to fly.  The monk watched in sorrow as the moth struggled in vain. It soon became clear that the premature intervention had left the moth's wings and body underdeveloped and full of fluid. The struggle to break free from the cocoon was essential for the moth's wings to gain strength and for the excess fluid to be squeezed from the moth’s body.
Reflecting on the unintended consequence of his compassionate act, the monk realized that the struggle was a vital part of the moth's transformation. In trying to alleviate its immediate challenge, he had unintentionally hindered the natural process necessary for the moth's survival. As the moth's life flickered away, the monk bowed his head in remorse, understanding the profound lesson the universe had imparted through this delicate creature. He realized that sometimes, the hardships and struggles we face are intrinsic to our growth, resilience, and the development of our inner strength. The story of the monk and the moth served as a reminder within the monastery. The monk acknowledged that the intricate dance of life often requires a delicate balance between compassion and allowing the natural course of events to unfold. Closing Thoughts We have to struggle and people we care about have to struggle. Often, it is more loving and helpful to tolerate and encourage the struggle instead of trying to alleviate it. Being willing to accept and find the lessons in the struggle fosters resilience over time, covering our feet in leather in a world that will never be totally soft. Forgive me for the woefully incomplete treatment of this idea. I wanted to get this into the mix of my blog topics so I can think about how it integrates with my other ideas.
Psychotherapy, at its core, can be seen as an application of philosophy, with different therapeutic modalities embodying specific philosophical perspectives. Somatic therapy can be thought of as applied phenomenology, in particular, where we focus on experiences manifesting in the moment. The philosophy of Phenomenology is reflected in somatic therapy in that it focuses on the subjective in-the-moment appearance of phenomena to an individual. This essay explores the relationship between philosophy and empiricism in the context of somatic psychotherapy, examining how these seemingly divergent approaches coalesce to create synergistic results. Philosophy in Somatic Therapy: Somatic therapy, which reflects the philosophy of phenomenology, partially operates on the premise that experiences emerge spontaneously in the present moment. Much like phenomena appearing in real life in phenomenology, somatic therapy delves into the immediacy of bodily sensations, movements, and experiences. This emphasis on the subjective, lived experience aligns with the phenomenological exploration of consciousness and the essence of experience. In other words, in somatic therapy, we avoid trying to interpret a topic of interest and instead focus on recreating the elements of it that we can in the room (i.e. through the use of projective objects and observing the body along with the emergent elements in the mind like spontaneous images). Antithesis of Empiricism: The immediacy of experiences in somatic therapy is antithetical to empiricism, which emphasizes observable "evidence" that there is a consistent "truth" across contexts that we can obtain through systematic evaluation, that is, the scientific method. While empiricism seeks tangible and measurable outcomes, phenomenology, particularly in the somatic context, values the subjective and spontaneous nature of human experience that invites the meaning-making of the person who experiences it. This inherent tension has historical roots, with empiricism initially appearing to be at odds with phenomenological and somatic approaches in turn. Synergy in Somatic Therapy: Despite the apparent dichotomy, modern somatic therapy demonstrates a unique synergy between phenomenology and empiricism, a combination that can be described as "toward" pragmatism as outlined in this beautiful essay by O.G. Rose. In a somatic therapy session, the subjective immediacy of phenomenological experiences is harnessed, providing a rich landscape for exploration. Empiricism, with its systematic evaluation, then complements this process by validating and verifying the generalized efficacy of somatic interventions. Furthermore, traditional evidence-based approaches bolster the efficacy of somatic therapeutic processes by acting as a measuring tool for how well someone is progressing in therapy as well as contributing valuable psychoeducation that orients the client. Together, they contribute to a holistic understanding of the human experience. For example, concepts like ‘formerly helpful belief systems that are no longer adaptive and cause problems for clients’ are core tenets of cognitive therapists. In the paraphrased words of one of my Sensorimotor Psychotherapy Trainers “cognitive therapies are necessary but not sufficient for genuine psychological transformation.” A client may know that they have faulty thinking but a part of them still holds that outmoded belief, along with its emotions and behaviors. Thus, when somatic therapy supports that part in transforming, we will have accomplished the goal that cognitive therapy sets out to do but is unable to provide in certain cases with its current set of tools and approaches. We need cognitive therapy’s goals and objectives so that we know we are on the right track with the somatic therapy. When both clients and counselors alike know what we want to accomplish and why, we are empowered by having direction and clarity and held accountable by grounded, empirically demonstrated measurements. Evolution of Empiricism's Perspective: Historically, evidence-based practices have been skeptical of working with the type of emergent material that somatic practices embrace. Emergent parts, memories, emotions, and the expression of these in the body were treated as things about which to educate the client, provide a cognitive framework to apply to oneself, and simply see how one’s logic is faulty, which was thought to be enough to provide a behavior change. However, certain enclaves of empirical researchers, like the presenters at the Interpersonal Neurobiology Conference, have shifted their stance over time, recognizing the value of phenomenological approaches in somatic therapy, primarily because we now have much better frameworks for understanding how psychological injury, a.k.a. trauma, functions in the nervous system. The integration of these perspectives has broadened the therapeutic landscape, allowing for a more nuanced understanding of the mind-body connection. Phenomenology Ahead of Empiricism: Within the somatic and other fields of study, phenomenology often outpaces empiricism in capturing the intricacies of human experience. In the study of the history of science, it is evident that experiments are inspired by how life appears to researchers. For example, Newton observed the apple falling and was inspired to create thought experiments that lead to the invention of calculus. He says in his letter to a friend named William Stukeley: "...the notion of gravitation came into my mind. All of a sudden, the apple, as far as I can make out, left the tree. Why should that apple always descend perpendicularly to the ground, thought I to myself. Why should it not go sideways, or upwards? But constantly to the earth’s surface... the reason is, that the earth draws it. There must be a drawing power in matter." The immediacy and subjectivity of somatic practices, such as emotions expressed in the body or images that appear in the mind eye, provide individuals with profound insights into their embodied existence. The manner in which these transformative insights are gained by means of somatic approaches has preceded and is in some instances still ahead of empirical validation, showcasing the unique ability of phenomenology to explore uncharted territories of the mind-body connection and other aspects of life. Of course, there is a long history as well that our interpretation of phenomena leads us astray. Therefore the eternal dance of phenomenological exploration and empirical validation is necessary for us to continue to approach “Truth…” or something like that. Challenges and Growth: While somatic therapy being ahead-of-its-time creates challenges in the field insofar as many of our approaches have yet to be empirically validated, it also prompts growth and innovation. Pioneering somatic therapists continue to explore new techniques and approaches rooted in phenomenological principles, pushing the boundaries of empirical research. This dynamic relationship fosters an evolving and responsive field that prioritizes the immediate needs and experiences of clients. In conclusion, the interplay between philosophy and empiricism in somatic psychotherapy reflects the dynamic tension between the immediacy of phenomenological experiences and the systematic evaluation of empiricism. Somatic therapy, as applied phenomenology, attempts to capture the essence of human existence in the moment, challenging the conventional boundaries of evidence-based practices. The evolving relationship between these two perspectives highlights the importance of embracing both the immediacy of experience and the empirical validation in the pursuit of a comprehensive and effective therapeutic model. Content Warning: This article discusses ideas that may not be suitable for someone who is early on in their therapy/self-healing journey and is more geared toward clinicians as well as clients who are ready to hear more about the intricacies of how therapy works.
Effective therapy is a balance between the “Magic” of deep dive processing modalities (like Sensorimotor Psychotherapy, MFR, EMDR, IFS, and other bottom-up internal process-based approaches) and the “Spinach” of doing hard work (studying, working out, applying yourself, etc), facing fears, sitting with grief, regulating anger, learning about faulty thinking, and recognizing that some current modes of being are no longer helpful (as in CBT, DBT, and other top-down (brain to body) systematized approaches). I am intentionally oversimplifying the intricate nature of the therapeutic process to shed light on a heuristic (framework for thinking about something) as I discuss the "Magic/Spinach" dynamic. Making "spinach" changes means having to feel some productive shame (although shame certainly comes up in the "magic" processes, too). I got the term “Spinach,” which refers to rote work and doing hard things, from Harvard professor of happiness Arthur Brooks. Love it. Before I continue, I am going to take a pause and discuss how shame can be productive: The concept of "productive shame" refers to a perspective where the experience of shame is channeled in a way that leads to positive outcomes and personal growth. While shame is generally considered a negative and distressing emotion, shame can also be viewed as a potentially transformative force when navigated effectively and in the appropriate context. Here are some ways in which shame might be considered productive in a therapeutic context: Awareness and Insight: Experiencing shame can bring attention to underlying beliefs, values, or behaviors that may be contributing to distress or maladaptive patterns. It can serve as a signal that there is something important to explore within oneself. Motivation for Change: Feeling shame about certain behaviors or aspects of yourself may motivate you to seek help and make positive changes in your life. The discomfort of shame can act as a catalyst for personal growth and self-improvement. Fostering Empathy: Experiencing shame can enhance empathy for others who may be going through similar struggles. It can create a sense of connection and understanding, both within oneself and in relationships with others who have faced similar challenges. Practicing Vulnerability: Acknowledging and working through shame requires a degree of vulnerability. Therapeutically, being able to share and explore these feelings can strengthen the therapeutic alliance and create a safe space for deeper emotional processing. Promoting Accountability: Shame can be a powerful force for promoting accountability. Taking ownership of your actions and their consequences, even if this accountability initially involves feelings of shame, can be a crucial step in the process of change and growth. Catalyzing Change in Belief Systems: Shame can prompt individuals to reevaluate and challenge their belief systems. The discomfort of shame may lead to a willingness to question long-held beliefs that are no longer serving them well. Cultural and Social Reflection: In some cases, experiencing shame may prompt individuals to reflect on societal or cultural norms that contribute to these feelings. This broader awareness can lead to social change and advocacy for more inclusive and compassionate communities. It's important to note that the term "productive shame" doesn't imply that shame is inherently positive. Rather, it suggests that within a helping context like therapy, acknowledging and working through shame can contribute to personal development and positive changes. Therapists must approach this aspect of therapy with sensitivity, empathy, and a deep humility regarding the individual's unique experiences and cultural background. Ok, back to Magic Spinach… or is it Spinach Magic? Anyhow: “Magic” refers to any modalities that provide what Bruce Eckert calls memory reconsolidation. Memory reconsolidation can be thought of as brain surgery by means of words. The therapist supports the client in opening their memory pathways that are trained on past wounds. The therapeutic dyad then reroutes those pathways by inserting reparative experiences. You can think of this as redirecting history as far as the brain is concerned. History itself does not change, but emotional aspects of the brain act as if history has, in fact, changed in a way. At times, clients experience a change in their belief system or behavior following as little as one session. It usually takes a few passes plus integration work to really make that change. It's so spectacular, you really need to experience it in the role of a client to see how strong the change can be. The original neural pathways of the wound never go away and can be triggered again but can greatly diminish in their ability to influence a person. “Spinach” refers to the work that reveals places where magic is needed and then helps the magic stick in the long run. There are a few different situations where the Spinach looks different. I will discuss two main situations: client in crisis and client who is stable but dissatisfied. If someone comes to therapy in a crisis, after we validate and regulate, the “Spinach” is looking at and acknowledging one’s part in the crisis as well as where one needs to let go of control and grieve. One’s part is anything that the person could reasonably take responsibility for and not something that was actually out of their control. On the other hand, someone might need to face and grieve existential realities like aging, death, loss, and random chance accidents. Facing pain and shame can be a challenging process, but it often leads to a sense of empowerment and the ability to make different choices. Some individuals may find themselves stuck in the validate-regulate-take ownership/grieve cycle for many years, continuously grappling with these challenges without reaching a point of empowerment. It's important to acknowledge that this phase can extend for a very long time and, in some cases, clients may not progress beyond the validate-regulate phase, and that's okay, but, unfortunately, feelings of empowerment in this instance might be scarce, which is not ideal. Empowerment is a product of taking ownership and/or grieving depending on what the situation requires. While all three actions—validate, regulate, and take ownership/grieve—are crucial, the emphasis on validate-regulate may persist for an extended period due to the need to address deep-seated wounds causing significant nervous system dysregulation. Initially, taking ownership may involve recognizing that the dysregulation is not the client's fault but is their responsibility.The process of taking ownership for life choices may occur later on. Take the classic example of an adult who was abused as a child. As a child they adapted to a bad situation. The adaptation was helpful and right at the time. Now, as an adult the adaptation is no longer getting the person the results they want or need. The adult must recognise that the adaptation was perfect in the past and came about due to bad circumstances. Here the adult will feel the scary feelings from the past, recognize them as “true” and regulate by coming into the present moment, recognising the danger is no longer present. Believe it or not, the process of updating the system can take years and decades. This process looks so simple and straightforward written out, but there are many trials, traps, and illusions that the adult must face as they come out of the past and into the present moment. Part of this process includes occasionally coming to terms with time lost to the adaptation, harmful beliefs, and, therefore, feelings of shame and regret that the person did not have more control over themselves. As a clinician, one can easily see that the mind prison that traps the client is not the client's fault, but just like the little child in the abuse situation, the adult once again blames themselves for problems outside of their control. Whether or not the person should feel shame and regret, they typically do at some point in the updating process. Even though the abused person left the abusive situation, they continue to choose people and situations that feel like the original abusive configuration. Jobs, friends, and partners perpetuate the conditions that created the mind prison in the first place, which not only continues to color the worldview of the abused but also deepens the neural pathways that reflect the impact of that abuse on the victim. Confronting the belief system of an abused person is a process that may span several years. However, I've consistently observed individuals in such situations reaching a crucial moment when they are finally ready to recognize their distorted worldview. The abused person begins to comprehend how the abuser's actions contributed to their belief system which led the victim to repeatedly choose similar situations in life. At this stage of therapy, the person has invested significant effort, enabling them to adopt a new belief system. Prior to this work, their nervous system dysregulation posed a barrier to such a choice. It's essential to clarify that the term "spinach" may suggest we are taking this lightly, but this confronting work is anything but casual. It can be the most challenging experience in one's life. Unfortunately, when the abused individual realizes they've been misled into this mindset, self-blame arises which becomes a period of shame and regret as they work to undo the damage. Consequently, shame, regret, and grief become an unavoidable yet natural part of the healing process. Moving on to situations that are post-crisis: Once the crisis and deep trauma have passed or a client comes to therapy because things are going well on paper but they feel “flat” or “blah,” that means the spinach is to encourage the client to “get stirred up” by doing something scary in their life that they have discussed wanting to do but are avoiding. That could be starting a business, pursuing a romantic relationship, adopting a suitable health regimen for themselves, etc. Basically, you support the client in introducing the pursuit of a major or minor life change that the client says that they want deep down but are avoiding due to a limiting belief system. Therapy sometimes takes on a more “coachy” feel, especially when using modalities such as CBT and DBT. In these methods, therapists offer clients an educational framework and employ motivational techniques to guide them in adhering to that framework. I believe it's crucial to incorporate goal setting and structured learning in therapy because solely focusing on the present moment process can lead to patterns of avoidance between clients and therapists. Clients may resist stepping out of their comfort zones to avoid potential triggers, while therapists might shy away from addressing client discomfort or distress, either due to a lack of understanding or a reluctance to confront areas of avoidance in their own lives. Striking a balance is essential to respect client autonomy, ensuring that encouraging clients to step outside their comfort zones involves a considerable amount of informed consent from the client. We never want to override resistance because it's there for a reason. Indulge resistance too much, however, and you wind up with conditions like agoraphobia and kindling (when triggers proliferate and become stronger rather than decrease in number and weaken). Facing fears is a skill. When someone comes to therapy traumatized, using compassion to help a client face fears in a controlled way is a top priority. As a therapist and not a coach, it is important to let go of the outcome of the client's actions. We are not so concerned with getting the client material world results like a coach is. Rather, we are observing how a client reacts to pursuing a goal or even the thought of pursuing a goal. When you are engaging in potentially triggering territory with a client, like goal setting, you must monitor for dissociation and other adverse reactions that indicate the client is too triggered, out of their window of tolerance, and needs support in decreasing the triggering stimuli. A client getting triggered by something is still useful, however, because it reveals the client's belief system; where there is a trigger there is an unhelpful belief and/or a wound to be processed. Is it better to find the wound and beliefs without triggering the client? For the most part, yes. But it is not the end of the world if a client gets triggered. At best, it's a rich learning opportunity and a moment where we can make some real changes if handled correctly. And so, we encourage the client to pursue a goal, the client begins to do so, gets triggered, and then we can swoop in with the magic of processing and begin memory reconsolidation, installing a new pattern. After this process, the client may realize they want the goal to look different from what was originally imagined. Often, something more in alignment with the client is determined, and the client successfully completes a similar but improved goal in the end. While the client pursues the goal, the therapist has to watch for when the client needs to be encouraged to face their fears (spinach) or if the client needs to process (magic). These two, together over time, create a positive feedback loop, ultimately launching our clients towards their dreams with as little time lost and, frankly, as little discomfort as possible. Again, therapists sometimes avoid supporting clients in pushing themselves because it's uncomfortable, but if you understand this positive feedback loop, you are drawn to empowering you clients in this way because you have confidence that your clients will potentially be able to extract themselves from the pain of avoidance and into the bliss of agency. The longer the client is in avoidance, the longer the pain is prolonged. Timelines may vary here so it is important to expect this process to take years or, at times, be impossible to complete. Therefore, this does not mean you are overwhelming your clients with pushiness. Rather, you are testing the waters regularly to find the best pace and direction for them. To recap, effective therapy can be thought of as threading the needle between the transformative "Magic" of deep processing modalities and the essential "Spinach" of confronting challenges and acknowledging faulty modes of being. The "Magic" involves memory reconsolidation, akin to rewriting emotional history, with the potential for rapid shifts in belief systems or behaviors. Meanwhile, the "Spinach" represents the hard work and processing of difficult emotions required to make these changes enduring. Whether addressing crises or encouraging clients to stir up their lives during moments of stagnation, therapists navigate a fine line between coaching and therapeutic interventions. Emphasizing the importance of facing fears and engaging in deep processing, therapists play a crucial role in steering clients toward their goals while remaining attuned to the balance of discomfort and growth. By understanding and embracing the positive feedback loop between "Magic" and "Spinach," therapists aim to guide clients towards agency and fulfillment, reducing the duration of pain associated with avoidance. This nuanced approach, avoiding undue pushiness and adapting to individual needs, creates a therapeutic journey that minimizes discomfort and maximizes progress over time. Unfortunately, humility sounds an awful lot like “humiliation,” and individuals can project a sense of “going to be punished” on the concept. However, a strong sense of humility is a marker of good mental health because when one is oriented towards reality, you can't help but feel humble.
What is Humility? Humility is a virtue characterized by modesty (i.e., not grandiose; properly estimating how much of one’s power enabled a positive or negative outcome) and a respectful attitude toward oneself and others. It involves an awareness of one's limitations, a lack of arrogance or excessive pride, and a willingness to acknowledge and learn from mistakes. Humble individuals tend to be open to different perspectives, value the contributions of others, and approach situations with a sense of curiosity and a willingness to grow. Humility does not mean self-deprecation or a lack of self-confidence. Instead, it involves recognizing one's strengths and accomplishments while also acknowledging that limitations will always exist and there is always room for improvement. Humble individuals often demonstrate a sense of empathy, gratitude, and a genuine interest in understanding and supporting others. Humility is often considered a key virtue and is seen as a foundation for personal and interpersonal growth. It can foster positive relationships, effective collaboration, and a continuous pursuit of knowledge and self-improvement. What’s not to love about humility? My faviorite thing about humility is how it helps us to relax and appreciate life. Humility contributes to a more relaxed way of living: Reduced Stress from Perfectionism: Humble people tend to be more accepting of their imperfections and mistakes. This acceptance can lead to reduced stress associated with the need to be perfect or constantly meet unrealistic standards. Openness to Learning: Humility involves a willingness to learn from others and from one's own experiences. This open-minded approach can alleviate the pressure of feeling like one must have all the answers, as humble individuals are comfortable with the idea that there is always room for growth and development. Lowering Expectations of Others: Humility often goes hand-in-hand with realistic expectations of oneself and others. This can prevent unnecessary disappointment and frustration when things don't go as planned or when people don't meet unrealistic standards. Enhanced Interpersonal Relationships: Humble folks are generally more understanding and empathetic, which can contribute to healthier and less stressful relationships. The ability to see and appreciate others' perspectives can reduce conflicts and promote a more relaxed social environment. Freedom from Ego-driven Stress: Humility involves letting go of excessive ego and pride. By not being overly concerned with how one is perceived or constantly seeking validation, individuals can experience a sense of freedom from the stress associated with maintaining a certain image. Embracing Uncertainty: Humble individuals are often more comfortable with uncertainty and ambiguity. Instead of feeling overwhelmed by the unknown, they can approach life with a sense of curiosity and a willingness to adapt to changing circumstances. Gratitude and Contentment: Humility is often associated with gratitude for what one has and a contented attitude. This gratitude can lead to a more positive and relaxed outlook on life. Humility allows individuals to approach life with a more balanced and realistic perspective, reducing the self-imposed pressures and expectations that can lead to stress and anxiety. It promotes a mindset that values personal growth, learning, and meaningful connections with others over the constant pursuit of external validation or perfection. Practicing mindfulness and being present in the moment can be supported by asking yourself certain questions. Here are some questions that can help you be more present:
The following are particularly good if you have habitually anxious or catastrophic thoughts and feelings (i.e. a chronically dysregulated nervous system):
The next set of questions is for presence in general and can serve as a practice to encourage more of a sense of “being here now centered in your body”:
These questions serve as prompts to redirect your focus to the present moment, strengthening your in-the-moment relationship to mindfulness and a deeper connection with your immediate experience. These questions encourage groundedness and centeredness. Psychoneuroimmunology (PNI) is a field of study that explores the interactions between psychological processes, the nervous system, and the immune system. The term is derived from three major components:
In essence, psychoneuroimmunology investigates how the mind and emotions influence the nervous and immune systems and how these interactions impact overall health. Researchers in this field examine the bidirectional communication between the brain and the immune system, studying how stress, emotions, and mental states can affect immune function and vice versa. The findings from psychoneuroimmunology research contribute to our understanding of how mental and emotional well-being can influence physical health and susceptibility to illness. It has implications for fields such as medicine, psychology, and immunology, providing insights into the complex connections between mind and body. What role do fascia and the interstitium play in psychoneuroimmunology? Fascia and the interstitium are connective tissue components in the body that have gained attention in various fields, including psychoneuroimmunology (PNI). While research is ongoing, here are some potential connections between fascia, the interstitium, and psychoneuroimmunology: Communication Pathways: Fascia and the interstitium are involved in communication within the body. They provide a network that allows signals to be transmitted between different tissues and organs. This communication system may play a role in the bidirectional communication observed in PNI, where psychological factors influence the immune and nervous systems. Inflammation and Immune Response: Both fascia and the interstitium are associated with the regulation of inflammation. In PNI, chronic stress or psychological factors can contribute to inflammation, and understanding how fascia and interstitial tissues are involved in immune responses may provide insights into the link between mental states and immune function. Neurotransmitter Release: Fascia contains sensory receptors, and the interstitium has been found to contain nerves. These structures may contribute to the release of neurotransmitters and other signaling molecules. The communication between the nervous system and the immune system, a key aspect of PNI, may involve these tissues. Tension and Stress Response: Fascia is involved in providing structural support and maintaining tension in the body. Chronic stress or psychological tension can affect the fascial system. Understanding how changes in fascial tension relate to stress responses and the subsequent impact on immune function is an area of interest in PNI. It's important to note that while these connections are being explored, understanding the precise roles of fascia and the interstitium in psychoneuroimmunology is still an evolving area of research. The interplay between psychological factors, the nervous system, the immune system, and connective tissues is complex and multifaceted. Finding metanalyses to cite this information directly is not available since this line of research is so new. The following are a few examples of where these conclusions/hypotheses are being drawn. Ball, T. M. (2011). Structural integration-based fascial release efficacy in systemic lupus erythematosus (SLE): Two case studies. Journal of Bodywork and Movement Therapies, 15(2), 217–225. https://doi.org/10.1016/j.jbmt.2010.10.006 Lupus is an autoimmune disorder. Though this article explores this one disorder, there are many other articles that explore the role of fascia and autoimmune processes. Bordoni B, Zanier E. Clinical and symptomatological reflections: the fascial system. J Multidiscip Healthc. 2014 Sep 18;7:401-11. doi: 10.2147/JMDH.S68308. PMID: 25258540; PMCID: PMC4173815. The Bordoni article talks about mechanical stress and inflammation’s role in interacting with the fascia system. I would argue that psychological stress is the same as mechanical stress because people generally tense and brace against stress. Bracing and tensing happen in the muscles and fascia, adding mechanical stress to the body. Poshattiwar RS, Acharya S, Shukla S, Kumar S. Neurological Manifestations of Connective Tissue Disorders. Cureus. 2023 Oct 16;15(10):e47108. doi: 10.7759/cureus.47108. PMID: 38022020; PMCID: PMC10646945. ^ This is an article that explores the connection between neurological and connective tissue functions, albeit by means of pathology. Gabor Mate, especially his book “When the Body Says No”, is a great resource for a more narrative exploration of PNI and the manifestations of “dis-ease” that result from stress. Exploring the connection between the fascia, psychology, neurological activity, and immunological processes provides an increasingly clear lever for healing trauma, its many challenging health manifestations, and a pathway forward to a sense of well-being in general, trauma or not. Ultimately, this budding research encourages us to keep moving, stretching, breathing, and developing our powers of attention and consciousness.
Here is an article by Robert Schelip on the way that fascia senses. He covers the five major nerve endings (Golgi, Ruffini, Pacini, the muscle spindles, and the interstitial free nerve endings) and how each can be stimulated to cause tissues to release.
He summarizes the takeaways at the end of the article:
Understanding how to relax and release fascia is important for not only healing from trauma but also for optimizing a sense of wellness and wellbeing. Think about a time you felt truly well. What did you feel in your body? People usually talk about feeling relaxed, strong, at ease, connected, and confident. Having a great deal of tension and lack alignment in your tissues can offset a feeling of ease and strength. When you approach trauma healing or even the pursuit of feeling your best, it is wise to consider your fascia because when your fascia is restricted or atrophied, you feel the sensation of that. it becomes a chicken or egg scenario. Are my emotions affecting my tissues or are my tissues affecting my emotions? It's important to take an inclusive view here. As we age we all approach a greater likelihood of chronic illness. Some of us start to experience the breakdown of the body much earlier than that. That does not mean we have to live with "dis-ease," however. For example, I have had chronic nerve pain off and on since age 16. Today I am a little over 6 months postpartum. It's no secret that pregnancy and birth is hard on your body. My nerve pain has been particularly loud lately, so I have my fascia on my mind more than usual these days. My pain comes from misalignment in my tissues. I use a variety of fascia strengthening and releasing techniques along with nervous system regulation exercises. Not only do I experience the realignment of my body as I rehab my system, I also experience waves of emotional release and nervous system discharge. I feel grateful for my education in bodymind regulation because, even though the regulation process can feel uncomfortable sometimes, I understand why I am feeling what I am feeling and can get to a calm, connected, and strong place quickly and reliably without having to cope or to deny my difficult feelings and sensations. Furthermore, fascia focused practices provide a surprising result. Even when I am out of alignment or in pain I still feel able to find that calm, connected, strong energy. I no longer feel that my sense of wellbeing hinges on being pain free or not having an emotion to process. I can stay connected to beauty and meaning no matter what I am experiencing in the moment. How interesting! As I learn to balance and regulate my bodymind, I feel less attachment to having everything sorted out inside. There is more of a sense of space and ease no matter what life throws at me, inside or out. I just found this essay I wrote back in June of 2022. As you explore the inner world of yourself and others, you will see there is a sort of underlying 'first principles' or rules from which our organization emerges. Give Them Some Oxygen 6/2/2022 Embracing the Hidden Wisdom Within: We all have parts that we don't like and try to smother. Parts that hold emotions that we reject, like anger, hate, weakness, sadness, shame, and wild pleasure. When we smother these parts, we dissect ourselves into arbitrary borders and dub some worthy and others unworthy. We become polarized and lose sight of what is wise about these othered parts. The Cost of Categorization: We do this because we feel those parts are costly. In our attempts to decrease our vulnerability, we become polarized in our thinking. We make some parts “good” and others “bad.” It is the categorization and labeling of these parts that is the origin of all functional mental illnesses. The parts that get smothered don't die, nor do they grow weaker, they instead struggle against their restraints and gag. They pop out sideways, acting out and demanding freedom to enact their wisdom. Reclaiming Wisdom: It's true that the unbridled expression of many of the parts that we reject, we learn to do because their expression was costly at some point. In our time of low understanding and lack of support, we make up stories about these parts so that they can never do the damage that they had done in the past. Ultimately, however, those urges that those parts have are wise in some way. They are pointing to something that we need either from others or from ourselves. As we mature and gain understanding and resources, someday, we can relieve the gag order and give these parts some oxygen. When we give these parts oxygen, it can be really scary. When those parts come, we feel the emotions that come with them. Perhaps there's hate, perhaps there is rage, perhaps there is a kind of blissful Mania that has no place in our home or business. When these parts come in, we feel those feelings we get scared that maybe we'll get stuck there, maybe the power I gained over this part will go away, and I will be overwhelmed by it. So, of course, in the beginning, it's important to do it with support, like Virgil holding Dante's hand in the Underworld. The Alchemy of Self-Discovery: We need someone who knows what they are witnessing to coach us through the intense sensation of the part as well as the intense reaction that we tend to have to that part. And with our hands held in this way, we are able to finally or at least start the process of seeing what this part is all about. And when we finally give this parts some oxygen, we begin to understand. Oh! We can hear the wisdom of what this part holds that we locked away when we locked away the dangerous aspects too. We get the opportunity to sort out that which is useful and that which is costly. In that sorting, this part has the opportunity to alchemize and transform into something updated that we can use now in our present lives. Trusting the Allies Within: We begin to see our parts as a gaggle of children in our charge. Never wanting to smother or deprive any of them but rather to lovingly understand and listen to the fate-altering, mind-blowing information that they have for us. And in so doing, finally, we get to reap the benefits of all parts of ourselves, updated and shown where we are now in our lives. We learned to trust these parts and give them access to the viewing room of our world. And when they see what we have become, they grow up to become whatever it is that we and they need them to be. We stop seeing these parts as enemies and instead see them as allies. We make amends for the misunderstanding and the defamation that we perpetrated on these sweet little beings.   I originally got this metaphor from my mentor, Steve Finn. Thanks, Steve!
Think of your emotional capacity like a bucket that can only hold so much. Everyone has different-sized buckets, and buckets can grow and shrink. When this emotional bucket overflows, it can lead to various reactions, from feeling depressed to getting anxious to getting angry. This post explores the importance of understanding these emotional limits, what happens if we ignore them, and the steps to help us recover. Inside the Emotional Capacity Bucket - Limits and Reactions: Everyone has a limit to how much stress they can handle and must find the right stress balance. Lack of “good” stress is also a form of “bad” stress, but that's for another article. Going beyond this limit can make some people feel sad, while others might get mad. In extreme cases, it might make someone think about making big changes in their life, like leaving their job, filing for divorce, or even suicide. Accumulating Stress: Once the emotional capacity bucket has been maxed out, every new stressor adds water to the emotional bucket, bringing you closer to “overflowing.” Even good stress pushes the person closer to the edge. People react differently to stress, so it's important to recognize that each person has their own limit. Expecting someone to behave or have the same capacity as you is misguided. Coping Requires Emotional Strength: Figuring out how to deal with problems requires emotional strength. If you’re already overwhelmed, it can be hard to express what you need or want. This is why typical “fix it” or “bootstrap (do-it-yourself)” interventions don’t work when someone is maxed out. Has anyone ever given you a lecture on mindfulness or told you to “take deep breaths” while you were overwhelmed? Or maybe they started giving you solutions saying, “Well, if you just did ‘xyz,’ you probably wouldn’t be feeling this way.” How did that feel? I personally believe coping should be used sparingly because it is much more efficient and effective to validate and allow difficult emotions to process through rather than trying to quell them with coping strategies. “Quelling” or soothing is really just gentle dismissing. Allowing emotions to process unburdens the person. The therapist or friend acts as a saucer who catches the overflow from the emotional capacity bucket. Listening and validating are the tools that help the excess water out of the bucket into the saucer of the person with more capacity in that moment. The beautiful thing about receiving the support of a good “saucer” is your bucket's capacity grows. Not only do you get relief in the moment, but you also are less likely to be overwhelmed by the same things in the future because you had the experience of surviving the hard situation and were supported enough to digest and reflect on what was hard about it. When you encounter something similar, your body and nervous system draw on the memory that you got through it before while in connection with a caring other. The embodied felt sense of that connection makes your emotional capacity bucket bigger, often even when no one is around. I want to note that in a world where good "saucers" and people with large buckets are limited, the vast majority are coping. I agree with Hafiz: “Fear is the cheapest room in the house. I would like to see you living In better conditions.” ― Hafiz Seeking Therapy Requires Emotional Strength: Telling an overwhelmed person to “just go to therapy” is harmful. Going to traditional psychotherapy requires some wiggle room in the stress bucket. If someone is already dealing with a lot, therapy might not be as helpful. It's a bit like trying to teach someone to swim when they've fallen off a boat—it might not be the right time. Getting bodywork that is focused on relaxation, neurofeedback, or supporting the person in carving out time for exercise, forest bathing, or alone time to do whatever they want can be much more helpful. Somatic Trauma and Attachment Therapists know how to work with the body without speaking and provide a viable alternative to traditional therapy for an overwhelmed person. See Emotional Injuries Like Physical Injuries When someone’s nervous system is maxed out and their bucket overflows, you must treat that person’s emotions like a broken bone or like the person who fell out of the boat in the earlier example. It is much harder for people to see emotional injury the way we see physical injury, but they are the same and often impact the nervous system similarly. Once you see it this way, you will feel silly if you find yourself arguing, dismissing, lecturing, or explaining to someone with an emotional injury. It will feel the same as arguing, dismissing, lecturing, or explaining to someone with a broken bone, like so: “Why are you crying? Everyone breaks bones. Don’t be such a drama queen.” “Why are you crying? Everyone gets anxious. Don’t be such a drama queen.” “Why can’t you help me with the groceries? It’s only a little broken.” “Why can’t you help me with the groceries? You’re just a little stressed right now.” “You know, I broke my arm once, and I was fine with it. It really made me a stronger person overall.” “You know, I had a panic attack once, and I was fine with it. It really made me a stronger person overall.” “Well, if you had paid more attention and not let things get out of hand, you wouldn’t have broken your bone. I’m not sure I want to take you to the ER. You need to learn your lesson.” “Well, if you had paid more attention and not let things get out of hand, you wouldn’t have become suicidal. I’m not sure I want to take you to the ER. You need to learn your lesson.” “Aw, come on, don’t complain about your broken bone. How do you think I feel?” “Aw, come on, don’t be angry. How do you think I feel?” “Oh wow! Your broken bone hurts so bad you've been in bed for days. Have you tried breathwork?” “Oh wow! You’re so depressed you've been in bed for days. Have you tried breathwork?” “You still have chronic pain? You’ve had that for 18 years! You should just get over it.” “You’re still sad about your childhood? You’ve been an adult for 18 years! You should get over it.” If you're the person with more emotional capacity, you may be thinking, “Well, it's not MY responsibility to coddle the emotionally injured person! What if I give in to their theatrics and make them weaker?” That is exactly the point I am making here. Validating and helping the person process the emotion makes them stronger. Dismissing and denying makes them weaker. You are actually making more of a problem for you and them down the road by trying to get rid of their problem rather than treating it like the injury that it is. It is the same as ignoring a broken bone. If I ignore a broken bone, it heals in such a way that the bone is weaker and more likely to break again. If I try to use the limb with the broken bone before it is healed enough, I reinjure the bone, and the recovery time is longer. Recognizing the Need to Stop: When something is wrong with our mental health, the first step is to recognize it and take a break to figure things out. Just stop. Then observe. That pause is so important. It can feel like swirly chaos, nauseating, clenched, imploding, exploding all at the same time. This is why people avoid stopping, but it is 100% necessary. Then observe. Take on a beginner's mind. Watch how you think, feel, and behave without trying to make any changes at all—just notice. Take the Pressure Off: Just like we wouldn't put weight on a broken leg, we should avoid things that add stress to our minds during the recovery time. Clear your schedule if possible. Taking medication might be a good idea. If you have to work, do the bare minimum. Take as many goals and deadlines off your plate as you can. Focus on the present moment for the most part. You may need to update your identity. The sooner you can take the pressure off, the sooner you will be able to reengage with life. The clients I have worked with who can stop quickly (and quickly is usually a six-month process!) have less to recover from because the pressure has not been piled on top of being totally maxed out for years or even decades. Clients who have been maxed out and who have had to “carry on” in that state with added pressure to “keep it together” take a lot longer to heal. I often have to sell stopping to people because social pressures to perform, achieve, and produce make people who stop feel shame. Choose the Right Professionals: Seeking help from professionals, like talking to a doctor for a broken bone, means working together to figure out what will help. It is important to find someone who understands the power of listening and validating. It does not matter how many degrees, how much clout, how many fancy techniques or medicines they wield. If your provider does not listen to you, they will waste your time and cause a lot more damage. If you feel ignored, dominated, or dismissed by your provider, leave immediately. This can be so, so, so hard when you’re already emotionally maxed out. You may not be able to do it, and that’s ok. Once you can muster the strength, start interviewing other providers. How you feel with a practitioner matters. Taking Small Steps to Recover: After taking a break, it's important to take small steps toward feeling better. This is like doing exercises to help a broken bone heal. You should move to this phase only once the bone is strong enough to do gentle physical therapy. On the other hand, not moving to this phase when it is time is also injurious. There are a lot of reasons people might avoid moving on to the active recovery phase:
Make Intentional Life Changes to Stay Healthy: Once the gentle recovery process has begun and we start to feel better, we can start to think about overall changes to make in our lives. Intentional changes that begin to emerge as a part of the healing process come with the belief: “Something wasn’t working, and I have agency to live a life that works for me.” Intentional change takes into account ongoing stressors like chronic illness, demands of your culture, needing to work, paying down debt, and other facts of life that might be present for you. Intentional change does not come from a place of ignorance or naivety. Rather, it takes stock and inventory of what is true now and what is possible from here. This differs from the changes made during a crisis. Changes made during a crisis often involve projecting all of the “bad” and blaming one person or situation or making broad sweeping generalizations about all of life itself (which can lead to suicide). Changes made during a crisis come with a belief that “if I just get rid of this one thing, it will ‘throw-away’ all the bad stuff in my life.” Understanding and respecting our emotional capacity is not only a personal responsibility but also a collective endeavor to develop a culture that truly understands and prioritizes mental well-being. Through awareness, validation, and intentional actions, individuals can navigate the complexities of their emotional worlds, promoting resilience and creating a foundation for lasting positive change. "The only way to make sense out of change is to plunge into it, move with it, and join the dance." - Alan Watts
Why do I keep getting into abusive relationships? Why do I stay in a job that I hate? Why do I keep choosing addiction when I know that I really want connection? I need to change, but I am scared and frozen. Why is that? Ancient Fear Human fear of change is a complex and multifaceted phenomenon rooted in evolutionary, psychological, and sociocultural factors. Avoiding change helped our early ancestors survive. They were much more subject to rapidly and dangerously changing conditions and needed to seek security to survive. Our ancestral instincts are incompatible with the conditions under which we now live. The result is that modern people stay “frozen” unnecessarily, or even to our detriment, in habit loops, unable to move on to a more enjoyable existence. The following reasons for fear of change come from our harsh beginnings and the nature of human social relationships that developed to meet our original challenges:
It's important to note that the degree to which someone fears change can vary widely, and some people are more adaptable and open to change than others. Furthermore, the context and nature of the change play significant roles in shaping individual reactions. Regardless of your circumstances, embracing change is a practice that improves when we bring intentionality to it. How do I increase my capacity to change? “Fear is a mile wide, and an inch deep. We perceive it as a massive ocean. Then we step into it, we realize it's just a puddle.” - Leila Hormozi Increasing one's capacity for change involves a combination of self-awareness, intentional effort, and a willingness to embrace new experiences. In many ways, embracing change is going against human instinct. You are not less of a person for feeling insecure while going through change. Rather, insecurity is to be expected because resistance to change is hardwired into us as a species. Here are some strategies to enhance your ability to navigate and embrace change while managing the inherent vulnerability and insecurity of the change process: Process Freeze States:
Change is a gradual process, and it's okay to take it one step at a time. Consistent effort, self-compassion, and a willingness to learn can significantly increase your capacity for change. Sometimes, a sense of urgency and the desire to rush change is a way to avoid change. This can stem from a fear of the change process. The urgency is trying to skip over the painful parts of change outlined in the first list above. Change can feel like jumping off cliffs. You can develop your relationship with the change process by jumping off curbs instead of cliffs to start to get used to the feeling of “falling.” Facing your fears does not mean you must be frozen in terror or bowled over by overwhelming emotions. If you look at change with an experimental attitude, you can take the pressure off of being perfect. Experimentation invites and expects mistakes. It values mistakes and failures as the fastest way to arrive at modes of living and functioning that work best for the given moment in time. Expect Complex Emotions and Be Ready by Knowing Your Own Complexity Have you ever heard clients (or loved ones, if you’re not a therapist and want to participate in the exercise) say things like this? What are the underlying emotional states you see in each example? (Suggested answers are at the bottom of the article.) 1. “I just feel so much rage, I literally see red. Like my vision is covered in a red film.” She said, visibly shaking in her seat. “If my colleagues knew, I don’t know, I could lose my job, or worse, my reputation. I’ve done things I’m not proud of.” 2. “I’m bad…” he stares off into space, “evil. There’s evil in me. I feel like I deserve all the bad things that happened to me. It's hopeless; I’ll never get better.” he pauses again, “I dont know if I want to get better. I want to die and take the whole world with me. Burn it all to the ground, you know?” 3. “When I think about what happened,” they said grimacing, “I dunno,.. Ugh!” they stuck their tongue out as if to vomit and lifted their hands, repulsed “It's just so disgusting, it's unbelievable! I CANNOT believe it.” 4. “I think I hate him…I HATE HIM!” he exclaimed, suddenly stopping in his tracks like a record scratch. His eyes stared off to a corner in the room, and all the life drained from his face. His voice faintly floated out of his throat, saying, “Oh wow, I was so worked up, but now I have no idea what we were talking about.” In the world of therapy, emotions are complex and varied, often bringing forth a rollercoaster of feelings for clients. As a therapist, it's crucial to expect and embrace the full spectrum of emotions that clients may experience during sessions. Here, I will explore the importance of acknowledging and creating space for feelings such as shame, anger, sadness, vulnerability, confusion, disgust, and even suicidal ideation. We'll discuss why attempting to "fix," "soothe," or "dismiss" these emotions is counterproductive and explore the role of dissociation in emotional processing. Moreover, we'll discuss practical strategies for therapists to navigate intense feelings, incorporating somatics and parts work into the therapeutic process. Embracing a Range of Emotions: Clients seeking therapy may experience a wide array of emotions that are often considered uncomfortable or challenging. It's essential for therapists to anticipate and acknowledge feelings of shame, anger, sadness, vulnerability, confusion, disgust, and even thoughts of suicide. By expecting these emotions, therapists can create a safe and non-judgmental space for clients to explore and express themselves. As you practice, you will start to recognize the “aesthetic” of an emotional state. The aesthetic is a multifaceted experience of the person that includes thoughts, emotions, sensations, postures, movements, body tension and collapse patterns, images in the client's and therapist's minds, and more. Sometimes people refer to the aesthetic as the "energy" or "vibe." The ability to recognize the aesthetic enables you to determine what emotional state is present faster and to validate the client experience more fully. For example, I can reflect that a client is sad because they are tearful. If I have a more complex relationship with aesthetic and I am attuned to the overall aesthetic of "sadness" in this person, I can reflect a shift to sadness before the client is fully in it, which increases rapport and trust in that the client feels acutely tracked and also feels “felt.” Furthermore, not all clients cry when sad. Acknowledging sadness when the client's expression might be more subtle, or the person’s sadness is generally not recognized or honored, can increase the client's awareness of sadness and help the client feel safe to feel the sadness now and increasingly as time goes on. This goes for any emotion, especially socially “inappropriate” ones. Thus, we heal the consequences of death by a thousand paper cuts that shove emotions down underwater. Many people have not been explicitly told to “not feel that feeling” but have gleaned from their environment that it is not okay to feel certain feelings. This is primarily done through dismissing, fixing, and soothing. The result is like trying to hold a life raft underwater: 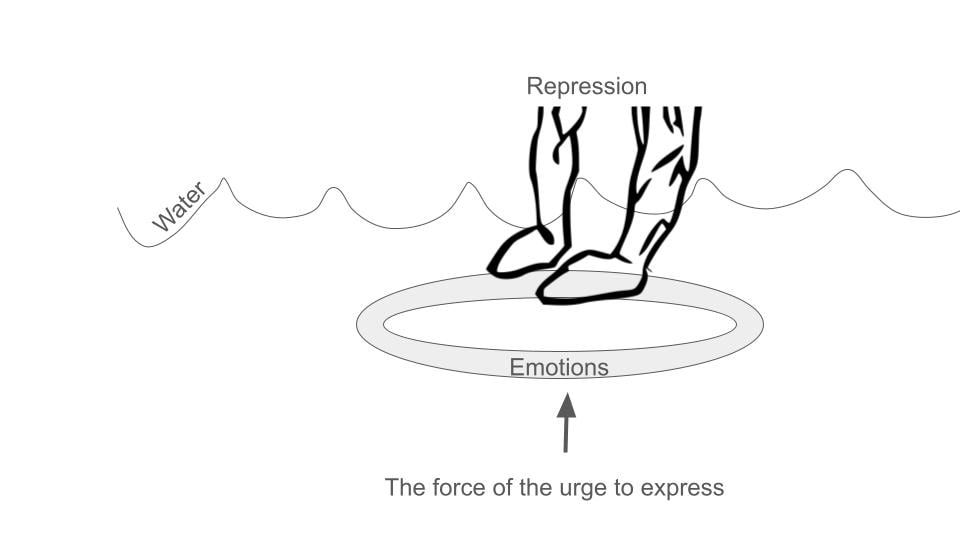 Avoiding the Urge to Fix or Dismiss: The impulsive reaction for many therapists, like those who trained the client not to feel in the first place, might be to alleviate their clients' discomfort by attempting to fix, soothe, or distract them from their emotions. However, these well-intentioned efforts can hinder the therapeutic process. Therapists should resist the urge to "fix" and focus on naming, validating, and feeling along with the emotions the client is experiencing. The exception to this rule is when a client dissociates; I will address that later. The reason that I see therapists have a hard time with this is that therapists have discomfort with their own socially unacceptable emotions. The only way for a therapist to get really good at validation is to be willing to feel fear, shame, disgust, and even suicidal ideation. The therapist needs to be unafraid to feel these feelings. Are you afraid to feel fear, sadness, loneliness, hopelessness, and the inner condition that causes suicidal ideation? If so, that means you don’t trust yourself to go into the emotional state and then come out of it. Another way to say this is that you don’t know how to regulate your nervous system at that level. Nervous system or emotional regulation does not mean that you are always serene and placid. It means that you can go into ANY feeling and efficiently find your way out. Ideally, what happens is the therapist feels a little bit of their version of the client's feeling, like rage, for example. Here’s how it goes down: The client looks tight; their jaw is clenched, biceps flexed, shoulder rounded forward, fists are starting to ball up, and their brow is furrowed as they talk about how, once again, their partner is making unreasonable, selfish demands. You say, “Wow! A lot of rage, huh?” Client: “Oh…my…god, I could punch a wall right now.” Therapist: “Oh yeah! Anyone would feel that way. I’m angry too hearing about this. Is it okay with you to feel this anger right now?” Client: “Yes, but I feel so stupid getting charged up like this.” Therapist: “Sure, that makes sense, you were taught it's not ok to be angry.” Client: “Right, anger was off limits. Mine was, anyway. What's the point of this anger anyway? It doesn't fix anything.” Therapist: “It's really uncomfortable to feel that much anger, huh?” Client: “Yeah, what do I do now?” Therapist:” What does your anger want you to know?” Client: “I am lonely and hurting.” Therapist: Oh yeah, can we just feel that loneliness and hurt together? Client: “Yes, that’s ok.” Therapist: “What’s it like to have someone feel this loneliness with you?” Client: “It's nice.” Therapist: “What's nice about it?” Client: “I do not feel alone; my anger can calm down. I feel like I can see my relationship in a different way.” This is an abbreviated example of validating, joining, and connecting the dots for the client and inviting the message of the feeling. There are many ways that this example does not capture how complex a dialogue like this can be, but the overall flow and format I present is something I experience repeatedly in sessions. Feelings are messengers. If we told the client to “try some deep breaths” when they wanted to punch the wall, we might not have arrived at the vulnerable feelings underneath. and we would not have been able to help the client feel connected. Notice how when the client feels connected and regulated, they can reframe their situation on their own. The therapist did not have to give them advice. This is the power of good implicit and explicit reflection statements, validation, and feeling with the client. It winds up being a lot less work for the therapist. Many therapists burn out, even in private practice, because they think they need to know everything or at least know a lot. Interpretive knowledge can help you steer the ship, but in actuality, you just need to know how to follow the client. That kind of knowledge is much less “expensive” than having to figure out how to interpret everything all the time. Understanding Dissociation: Many clients have learned that their feelings are not acceptable or valid, leading to dissociation as a coping mechanism. Therapists need to be vigilant for signs of dissociation, as it can be damaging if left unaddressed. Monitoring for dissociation and understanding its nuances is crucial for effective therapy. Rather than reacting to dissociation with panic or discomfort, therapists should strive to become competent and confident in handling it. Signs of possible dissociation include client reports and visible clues. Clients might report feeling confused, foggy, or suddenly feeling blocked while processing. Clients might not have words for what they are feeling, but you will get the hint they are dissociating because they suddenly look scared, frozen, or far away. Their speech may become slower, and more disorganized, their sentences might seem incomplete, or they may change subjects rapidly, becoming difficult to understand. It is important to know how to name the dissociation respectfully and artfully bring it to the client's attention. When a client dissociates, it means that something just “happened,” usually something that is “intolerable” for their system. Reassure the client that they always have consent and dont have to feel something they don’t want or aren't ready to feel. This reassurance can take the pressure off of the dissociation. I usually ask the client, “What was intolerable about what we were talking about just now?” Usually, the answer has something to do with “I’m not supposed to feel ______,” “I’ve trained myself not to feel_________,” “It’s too vulnerable to feel________,” etc. Rarely does a client recall a memory of which they weren't aware. Rather, it's usually an emotion or sensation that the client trained themselves not to feel long ago. Titrating Intensity with Somatics and Parts Work: To ensure the emotional intensity remains tolerable for clients, therapists can integrate somatic techniques and parts work into their practice. Somatics involves paying attention to the body's physical sensations, helping clients ground themselves in the present moment. Parts' work explores the various aspects of a client's personality or identity, facilitating a deeper understanding of their emotions without being consumed by them. The work, then, is to help the client learn to tolerate what has previously been intolerable. My aim with clients (and myself) is to be able to be present with any emotion or sensation. Once someone no longer has “off-limit” feelings, they experience much greater ease, clarity, and flexibility in life. It’s much easier to be continuously present. They can feel a feeling and efficiently find their way back to a healthy baseline, which is much easier to achieve if the therapist is constantly modeling regulation this way. It's a simple goal arrived at by a varied and nuanced path for every individual: Therapists play a vital role in helping clients navigate complex and challenging emotions. By expecting and embracing feelings of shame, anger, sadness, vulnerability, confusion, disgust, and suicidal ideation, therapists can create a supportive environment for clients to explore and express themselves. Avoiding the temptation to fix or dismiss these emotions, monitoring for dissociation, and incorporating somatics and parts work are essential strategies for therapists to foster a more profound and effective therapeutic journey for their clients.
Liz's Parts Work Journey
Studying non-dualistic spirituality in the tradition of Ramana Maharshi and my experience with clients during the first years in bodywork practice inspired me to see humans as multiple. Seeing humans as multiple contextualized a series of consciousness events I had growing up and in my early adult years. I am sharing this story because it highlights an underlying organization I feel in life. I believe that when someone discovers and interacts with this harmonious organization (aka spirituality, the "universe," the Game, the Tao, God, divine order and timing, etc.) in whatever way they name it, that the process of interacting with "it" is healing in and of itself. I discovered somatic parts work through a suggestion and a surprise. One day in 2010, my mentor, Steve Finn, told me, “Parts don’t go away, but we can throw them a retirement party or help them change their job description.” I adopted a “no parts left behind” policy from that day forward. At that time, I was also hyper-focused on non-dualistic spirituality from Ramana Maharshi's lineage and Eckhart Tolle's teachings. To see the good and the potential in others is a core tendency of mine, and this focus deepened my tendency to “see” the core essence of light and being in others. I have also been generally aware of the layers of disruption, anger, pain, and separation that layered on top of the core. The awareness of the layers increased at this time, too. I remember being confused as a young person because you couldn’t just interact with anyone and have an easy connection. I always felt like easy connection ‘should’ have been the case because I could “see” the core of perfection in others. Learning how the other “layers” or parts functioned helped me understand why the connection was so hard. Shift to Direct Communication with Parts As my clientele shifted to people with more significant trauma presentations, I began talking directly to parts. I would ask the parts and the client permission and invite the parts to speak freely. This was particularly easy with clients who had structural dissociation (the extreme version of this is called DID - dissociative identity disorder). It seemed to me that the parts needed someone willing to listen and go to the dark places with them. I was surprised that they tended to resolve on their own with good presence. I noticed that parts have their own postures and movement patterns, their own fascial restrictions, they hold disparate belief systems, and sometimes they even have their own mind/body dis-ease processes separate from other parts. Incorporation of Sensorimotor Psychotherapy (SP) My education in Sensorimotor Psychotherapy changed how I do parts work and added a new level of sophistication. I named my new Colorado-based therapy practice PROSOPON because I wanted to juxtapose the “prosopon” (πρόσωπον) or “parts that change,” i.e. masks or faces from the hypostasis (ὑπόστασις), “the essence that stays the same,” i.e. the non-dual core. This is one of the interpretations of this philosophical concept. (I also like how the “Os” in PROSOPON look like faces…to me anyway.) Philosophical Underpinnings and Education By the way, you see a lot of Greek and philosophy in my writing because I studied Latin for four years as a teenager and ancient Greek at my college, which is primarily a philosophy school (also called a great books program). I had the opportunity to study at the Zen Center in town concurrently. I am a great lover of evolving wisdom traditions and I bring them into my practice. Introduction to Internal Family Systems (IFS) I laughed out loud when I realized "how much time I wasted" (it's not really wasted time. The work was worth it and I wouldn't take it back for anything). I finally attended a 14-hour introductory course in Internal Family Systems this summer, the most recognizable version of parts work. I spent over 12 years developing my own approach when I could have just taken an IFS training. Fortunately, life is about the journey, not the destination. I took an introductory Janina Fischer training about her combination of IFS and SP (called TIST or Trauma-Informed Stabilization Treatment) this spring too. I must not have been ready to “get it.” I loved the training and incorporated what I learned, but it did not land like IFS. Accelerated Healing with Combined Approaches Incorporating the ideas of IFS, TIST, Sensorimotor, and my own style of approaching parts has accelerated the healing and recovery I have witnessed in my office. I am so excited to feel validated and educated by Dick Schwartz, his approach, and his community of therapists and trainers. The Implicit "Rulebook" for Parts Work The interesting thing for me is this: if I can develop my own version of parts work by interacting with client parts, as many therapists do, there must be an underlying implicit “rulebook” for how the human multiplicity of subpersonalities function. This reflects my experience with spirituality as well. When you simply turn your attention to something like the Tao, let’s say, over time, you start to get an embodied understanding of it that no word-based explanation can provide. The fundamental rule is that we are all multiple, and many of our mind-body and behavioral difficulties can be resolved if we start honoring, loving, and updating our subpersonalities as though they are real people. Key Modalities: IFS, Sensorimotor, and TIST I want to be really clear and transparent that I have yet to take level one of either IFS or TIST as of December 2023. I have taken introductory courses and studied material related to IFS and TIST, but I do not claim to practice these modalities per se. I incorporate my understanding of the philosophical and practical underpinnings of each modality. I love the IFS unburdening process because it's straightforward and user-friendly. Sensorimotor is magic surgery. SP properly applied manages a nervous system and its transformation better than any other modality I have ever witnessed. IFS helps SP get the job done by helping a client get to know their system, how to ask parts for genuine consent and learn about your non-dual core and how your parts relate to that core. The IFS framework creates an environment within which SP can do its magic. Importance of Regulation and "Titration" TIST highlights the importance of using parts for regulation and “titration” largely because Janina Fischer’s clientele, like mine, often have strong dissociation and overwhelm components. When an overwhelming feeling is present, we can't process it all at once. It's like being presented with a gigantic sandwich. I couldn’t eat the whole thing in one bite, but I can finish the sandwich if the bites are smaller and spread it out over multiple meals. When I recognize that an overwhelming feeling resides in just one part of me instead of all of me, it's like eating one bite of the sandwich rather than trying to choke the whole thing down. Pure Bottom-Up Somatic Work in Certain Cases There certainly are exceptions to this IFS and SP ordering. From time to time a client comes in, and they are so good at avoiding, or their nervous system is so disorganized that using emotional or sensing talk of any kind is unavailable. In these cases, I start with pure bottom-up somatic work, either myofascial release or somatic movement of some kind. Myofascial release is especially suited to help these clients because hardly any talking is required, and any talking that we do is related to purely physical things. Every time I have used this approach, the client begins to bring up emotional things on their own in their own time. You can read my article on trauma and fascia to understand more why starting with a pure MFR approach can be helpful for these presentations. I embrace the haphazard and, at times, comical nature of my journey (read “ignorance”), cherishing the continuous evolution of my 'selves' and therapeutic approach. The invitation to clients and clinicians is this: honor the journey, recognize the multiplicity within, and leverage the transformative power of somatic parts work. Trauma affects your fascia, but why should you care?
I care personally because addressing my fascia was key to my trauma-healing needs. I continue to regulate my nervous system with fascia care. I have seen the way my clients benefit. For some of my most complex cases, a course of hands-on fascia work allowed us to begin a healing process that sometimes ended decades-old symptoms. Clients have told me that the work can feel “psychedelic,” providing sudden insight, and “more relaxing than Xanax.” Those were just a couple of comments in the last few weeks. I could do a whole post on clients' reactions to the work (and I shall!). That seemingly simple body and touch work can produce effects as powerful as drugs without the hangover (usually) has completely altered my reality since I learned it in my mid-20s. It feels ordinary to me now, but I am constantly reminded of how amazing it is because my clients continue to react so strongly to it. “But why is fascia work so powerful?” you might ask. When I first encountered the power of fascia work, I asked this question, which kicked off a decade of voracious study on the topic. I will now attempt to give you a few distilled key points that can answer this question. The fascia and the nervous system occupy the same space in the body and are extremely intertwined. The fascia, a connective tissue, is intertwined with the nervous system as it contains sensory receptors called proprioceptors. These receptors provide information about body position and movement to the brain, contributing to the body's overall sense of spatial awareness. Additionally, fascia has been suggested to influence neural signaling and may play a role in conditions involving chronic pain or body system dysfunction (circulatory, digestive, lymphatic, immune, endocrine, etc.). Therefore, psychological trauma shows up in the fascial system. Psychological trauma can manifest in the fascial system through various mechanisms. Trauma may lead to increased muscle tension, affecting the fascia and potentially causing it to become tight or restricted. Chronic stress from trauma can contribute to the development of myofascial trigger points, which are hypersensitive areas in the muscles and fascia. Moreover, the body's response to trauma, particularly the fight-or-flight response, can create patterns of muscular tension and altered movement, impacting the fascial system. Emotional stress and trauma might also influence the autonomic nervous system, which can affect the fascia's tone and function. Research on the connection between psychological trauma and the fascial system is ongoing, and it's an evolving area of study within fields like psychoneuroimmunology and somatic psychology. Many of us in the Fascia and Somatic Fields regularly witness spontaneous memory recall when areas of an individual fascial system are released or when positions of past trauma (or even positions of neutral or pleasurable events) are experienced in a person's posture or body positioning. Fascial touch and movement techniques act on the Ruffini Endings and why that matters. Fascial release techniques, including stretching, “unwinding,” and a specific type of massage, may influence the fascia through various mechanisms, including stimulating Ruffini nerve endings. Ruffini endings are a type of proprioceptor found in the fascia that responds to sustained pressure and stretching. When myofascial release is applied, it can lead to a decrease in tissue tension and increased flexibility. The pressure and stretching stimulate Ruffini nerve endings, sending signals to the central nervous system that contribute to a relaxation response. This can result in a reduction of muscle tension and improved mobility in the fascial system. Since the fascial system is involved in all systems, including the nervous system, which is where psychological trauma is “stored,” trauma affects your fascia. Based on my personal, my colleagues, and my clients’ experiences, the current theory is that releasing fascia allows us to release some aspect of trauma stored in the central nervous system. Fascia also affects your trauma. The fascial system can put up to 2000 lbs per square inch on the body by means of restrictions that form in response to injuries and chronic psychological patterning. The brain registers this crushing force as danger and stress. When the circulatory, musculoskeletal, and other body systems no longer suffer the crushing pressure of fascial restrictions, they stop alerting the brain that they are in danger, thereby decreasing the overall stress load in the body. Big Caveat: much like mold illness, autoimmune disorders, and other stress disorders, while it is wise to treat restrictions at the body level (like treating mold symptoms through detoxification protocols), regulating your nervous system is ultimately more important. If you treat your restrictions without knowing how to regulate your nervous system, you'll be treating restrictions forever and wondering where is the benefit. Ideally, both happen at the same time. Why You Might Care. The profound interconnection between the fascial and nervous systems highlights the significance of addressing trauma through fascia care. The revelations stemming from personal experiences, as well as the transformative impact observed in clients, emphasize the potency of fascial work in trauma healing. The manifestation of psychological trauma within the fascial system, whether through increased muscle tension, the development of trigger points and chronic unexplained pain (think fibromyalgia and myofascial pain syndrome), or altered movement and posture patterns, emphasizes the intricate relationship between mind and body. The ongoing research in fields like psychoneuroimmunology and somatic psychology further validates the evolving understanding of how trauma “resides” within the fascia, so to speak. The tangible results witnessed by those in the Fascia and Somatic Fields, including spontaneous memory recall during fascial release, inspire hope in the potential of these techniques in unlocking and processing deeply embedded traumas. Fascial touch and movement techniques, by acting on the Ruffini nerve endings, offer a unique avenue for trauma release. The stimulation of these proprioceptors through pressure and stretching initiates a cascade of responses in the central nervous system, ultimately leading to a relaxation response. This process reduces tissue tension and enhances flexibility and mobility in the fascial system, which is intricately linked to all bodily systems. Thus, all body systems potentially experience renewed freedom in their function. In the process of trauma healing, the revelation that releasing fascia may facilitate the release of stored trauma in the central nervous system presents a compelling perspective. The comparison of fascial work to the powerful effects of drugs, without the undesirable side effects, speaks to the potential of this approach in promoting holistic well-being. As we continue to unravel the mysteries of the mind-body connection, the role of fascia in trauma becomes increasingly evident, providing new avenues for healing and resilience. 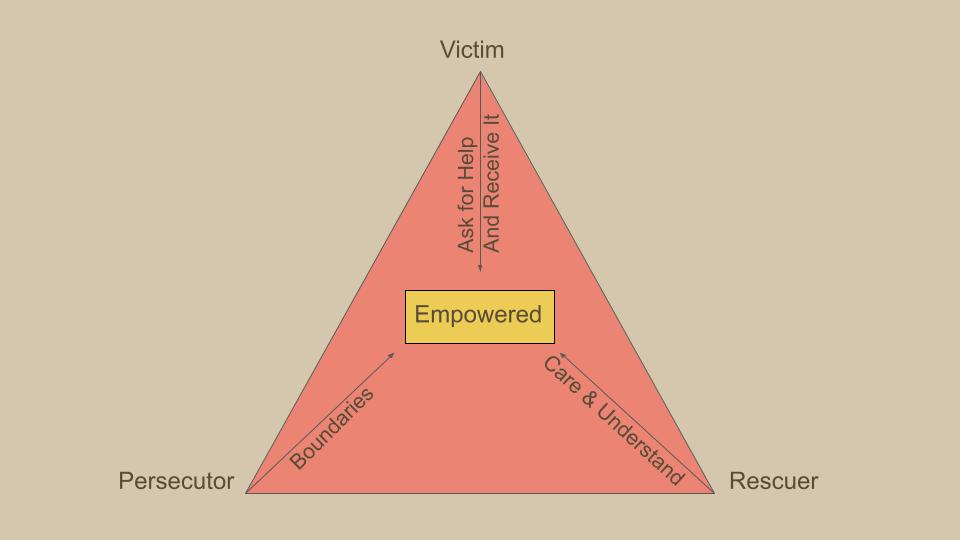 Karpman's Drama Triangle is a psychological model that explores the dynamics of interpersonal relationships and the roles people often unconsciously assume in conflict situations. Developed by Dr. Stephen Karpman, this model outlines three primary roles within the drama triangle: the Victim, the Persecutor, and the Rescuer.
This is a framework that clients often find helpful. Victim: The Victim in the drama triangle feels powerless, oppressed, or mistreated. They often portray themselves as helpless and may seek sympathy or external validation. Victims tend to avoid taking responsibility for their own circumstances and may inadvertently contribute to their feelings of powerlessness. Victims avoid personal growth by clinging to their victim status and blaming others.
Persecutor The Persecutor is the one who, consciously or unconsciously, takes on the role of the aggressor or antagonist. They criticize, blame, or attack others, creating an environment of conflict. Persecutors may feel justified in their actions and may not recognize the impact of their behavior on others. Persecutors avoid personal growth by devaluing and blaming others.
Rescuer The Rescuer is the individual who intervenes in the conflict, often with the intention of helping or saving the Victim. However, the Rescuer's actions can sometimes enable the Victim's sense of helplessness and may contribute to a cycle of dependency. Rescuers may also become frustrated if their efforts are not appreciated or if the Victim does not take steps towards self-empowerment. The Rescuer needs the Persecutor to persecute so that the rescuer can compare themselves to the persecutor and feel like a superior person. The Rescuer avoids personal growth by getting caught up in other people’s lives.
The Drama Triangle is dynamic, with individuals often moving between these roles in response to changing circumstances or triggers. What makes this model particularly insightful is its recognition that each role in the triangle can be disempowering and contribute to the perpetuation of interpersonal conflicts. Breaking free from the Drama Triangle involves individuals taking responsibility for their own roles and working towards more assertive, collaborative, and empowering communication styles. Doing so encourages self-awareness, accountability, and the development of more functional communication patterns. I am a fast processor, and I often attract fast-processing clients. People like us produce ideas rapidly. I also identify as a somatic person. I've spent a lot of time around people and groups that are intellectual and others that are somatic. Going through life as this combination creates dissonance. In somatic circles, I can be interpreted as disembodied. In intellectual circles, I can be interpreted as “out there.”
Internally, I feel congruent. When I observe misinterpretation, I notice it, feel a little disappointed, and reflect on how I truly feel inside. There is a temptation to get defensive. I want to explain myself. There is a misconception that you can’t be intellectual or a fast processor and simultaneously embodied. The truth is, you can presently embody whatever you are. You can even presently embody disembodiment. Speed has just as much a place in the body as slowness. Some bodyminds love speed. These body-minds often don’t do well with seated meditation and require other types of contemplative practice vessels. When you are choosing a contemplative style, choose one that feels good to you. White-knuckling through a 40-minute seated Zazen practice is not virtuous and misses the point unless your aim is to be present with limbic friction, which is also fine. Just be intentional that this is your aim. The point of a contemplative practice is to become present by repeatedly returning to a single focus. That could be a mantra or working on a Rubik's Cube. Your contemplative practice does not always need to be done as “time set aside” like a timed meditation. You could decide to return to your breath, sensations in your body, or something else, over and over while cooking or hiking in the woods. Doing focused timed practices is very helpful for learning presence and maintaining a strong connection to presence. If doing a timed practice is very irritating or brings up trauma, and that is not your aim, it's not time to have this as a part of your life. You may need some help from a therapist or spiritual person to work through your tangles inside. Once you have more inner clarity, you will love your practice in whatever form you connect with. Try a different practice if it feels like a chore or a battle. It might not be you. The practice vessel may be a bad fit. Types of Contemplative Practice Vessels:
What makes any of these practices contemplative is the quality of attention you bring to it. At first and in general, you practice keeping your attention on the thing you are doing. When your mind wanders, you bring it back. Over time, your relationship to contemplative practice evolves. You may feel an affinity for one specific practice vessel. Your preference may change to different practice vessels over time. It's important to know that it is not about any specific practice vessel (including seated meditation). The practice through any vessel is presence in the here and now. That is all. There is no aim other than this. The aim is not to “slow down,” “wake up,” “be better.” The aim is to be present and nothing more. “How can that be helpful?” You might ask. “Why would I want even to try this if it's not going to ‘help’ me?” Well, try it and see what happens. Let go of the mindful marketing out there that it's for this or that purpose, that you could become enlightened, or that you’ll be a better person. People have, understandably, used many tactics to convince others to do contemplative practices. They have used motivational and marketing hooks to get the job done. You may be reading this article because you want to be further convinced to practice. But why? Underneath all the teachings and mindfulness click-bait, there is something else entirely. I will not try to capture the “thing” or “not thing” in words. I can’t, and no one can. Lao Tzu famously points out the issue: The Tao that can be told is not the eternal Tao. The name that can be named is not the eternal name. The nameless is the beginning of heaven and earth. The named is the mother of ten thousand things. Try your hand at presence. Every time you do, invite total openness to what is. That is sensation, environment, inner experience, your life circumstances, the state of the world, that which you “know” and everything “you don't know,” and just see what happens next. If you're a fast processor or some other misunderstood type of person, don't try to “fix” yourself. There is nothing to fix. Be with who you are now and watch yourself become. Bodytherapy is Psychotherapy, and Psychotherapy is Bodytherapy.
There, I said it. This reality is a huge taboo, and its taboo status has been gnawing at me. Like many therapy professionals, my work is deeply connected to my personal journey. My life began with a foundation of confusion and fear, driving me to seek answers early on. At seven, I was fascinated by Maslow's hierarchy of needs, and by nine, I boldly declared that the cycle of my family's ancestral trauma would end with me. Despite having many friends and achievements, I always felt like an outsider, navigating life on shaky ground and unable to follow the "normal" path. My first encounters with therapy came during my teenage years, and I saw several psychotherapists in college. However, my condition continued to decline until I met a psychologist and an osteopath who treated me like a person. This, I believe, is the essence of good psychotherapy: seeing the client as a whole person. You might wonder, "If your other therapists weren't treating you like a person, what were they treating you like?" At times, I felt like I was merely a paycheck, a diagnosis, a problem, a juvenile delinquent, an ego booster, or a naïve teenager. I kept waiting for someone to ask, "And how does that feel in your body?" because I was experiencing so much physically, and I was surprised no one did. Working with those two professionals evolved into a mentorship that shaped my approach today. One helped me understand transference, countertransference, and parts work, while the other introduced me to Osteopathic Manipulation and Katsugen Undo. Both taught me mindfulness and spirituality, leading me to leave the traditional career path and start a massage and yoga practice. With their guidance, I moved away from medication, worked with a Functional Medicine doctor, and eventually stopped using FM protocols as well. By then, I had completed yoga teacher training, learned Myofascial Release, practiced energy work, and participated in extensive group therapy. I found freedom in using food, connection, and movement as my medicine, and for the first time in my life, I seldom felt fatigued because I was living in alignment with my values and regulating my nervous system. My clientele began to evolve, attracting people who had experienced trauma and were dealing with its psychological and physical consequences. During bodywork sessions, clients would sometimes shift into sub-personalities, discharge their nervous systems, or recall memories spontaneously. When someone becomes a scared two-year-old on your table, you help them. You don't tell them to "cut that out" because this isn't psychotherapy. I did my best but knew I needed more training. I attended the Interpersonal Neurobiology Conference and discovered Sensorimotor Psychotherapy. Shortly after, I woke up one morning and wept, realizing what I had to do. I shut down my thriving practice in Austin and moved to Boulder to study somatics. While in graduate school, I restarted my practice, earned my degree, and got certified in Sensorimotor Psychotherapy. I had the serendipitous opportunity to work with a Functional Neurological Disorders expert, which brought all of my education together, enhancing my ability to help others on their healing journeys. Learning to treat Functional Neurological Disorder (FND) was a pivotal moment for me, although I didn't realize it at the time. I hesitated to acknowledge it due to an unspoken taboo. Here's how this issue manifests:
I respect the needs of large mental health institutions and workplaces that train new clinicians. While graduate programs do have rigorous evaluation practices, they often fall short in screening out clinicians who misuse touch or power. Understanding why touch is particularly taboo in these programs would require further research. Do we doubt new clinicians' ability to discern which clients would benefit from touch? Or are educators reluctant to learn about the appropriate use of touch themselves? In residential programs, the taboo around touch is more understandable. During my time at inpatient treatment centers for people living with psychosis, it was evident that residents needed nurturing touch. However, allowing touch between patients posed risks, such as it turning into sexual contact or inappropriate boundary testing, which I witnessed frequently. While I believe we should strive to permit platonic touch despite these risks, I also understand why overworked and understaffed clinicians might avoid it. At a high-end facility for individuals with psychotic disorders, clients could leave the campus for massage therapy and physical therapy, among other complementary treatments. The disparity in care between those with and without financial resources is stark, and touch is one of the services these clients invest in. Integrating touch in certain sectors of the mental health field is indeed a complex issue. However, there are many settings where it is both feasible and beneficial, such as private practices, group practices, and some community mental health clinics with relatively high-functioning clients. I believe this enduring taboo around touch is more about habit than necessity, and it's time to reconsider these boundaries. We might need a separate field or license for those working with trauma from a nervous system perspective, or licensing boards could specify when and how such integrations are appropriate. Clinicians working in an integrated manner are generally not operating outside their license but are often fearful due to a lack of clarity. For now, I'll refer to this emerging field as Somatic Trauma and Attachment Therapy (STAT). STATs use:
STATs Treat
Somatic Trauma and Attachment Therapists (STATs) support individuals' personal growth and evolution while recognizing privilege and oppression dynamics and advocating for change in oppressive social systems. STATs receive education, training, and supervision from experienced professionals within the field. This outline represents the current boundaries of STAT practice based on extensive discussions with fellow STATs. I am passionate about continuing to explore and document the evolution of this field, as it is clearly developing its own unique path forward. 11/27/2023 Video + Article: The Difference Between Sensorimotor Psychotherapy and Somatic ExperiencingRead NowAs the regional organizer for Sensorimotor Psychotherapy, I often get asked what is the difference between SP and SE. I did not create either of these resources but these are what I give to people who ask that question. I, unfortunately, do not have the name of the person who wrote the article but I do know that they were certified in both SE and SP.
Comparison Sensorimotor and Somatic Experiencing Somatic Experiencing and Sensorimotor Psychotherapy are two very distinct therapies with differing goals. Their founders had different objectives in mind; Peter Levine wanted to learn how to heal human trauma from observing animals in the wild, while Pat Ogden wanted to synthesize body and talk therapies to heal traumatic and developmental wounds. As a result, there are fundamental distinctions in their notion of therapeutic action; their understanding of the role of feelings, words, and thoughts in treatment; and their ideas about the therapy relationship. For example SP has developed specific techniques for emotional and cognitive processing, which plays a very important role in SP treatment. In comparison, because SE it is an approach based on animal behavior, it does not treat higher order functioning in the same systematic way that it treats autonomic nervous system imbalance for which it has a highly developed protocol. The distinction in goals and intention is clearly reflected in the overall structure and content of the training programs. While some of the techniques are similar because both incorporate a neurobiological model, they are elaborated in very different contexts. In SP the techniques are taught in relation to broad principles of practice, phases of treatment, and stages of the therapy process. Students are taught to apply SP techniques in accordance with certain criteria, i.e. whether the trauma is developmental or shock trauma, whether the phase of treatment is stabilization or memory processing. In SE on the other hand, the focus is not on the timing of the application of the technique but on the refinement and enhancement of the individual’s capacity to discharge arousal through such practices as titration, pendulation, resourcing and managing over-coupling between different elements of experience. After the first level of training, SP and SE completely diverge. The second level of SP deals with attachment patterns and character strategies and processing resulting emotions and limiting beliefs. In the second level there is an elaboration of the relational focus of the model with an emphasis on transference, countertransference and enactments. In contrast, the second level of SE applies the principal techniques of the first level to distinct kinds of categorical trauma like physical injury, horror, inescapable attack, emotional trauma and natural disasters. Training hours are spent on specific traumas within these categories such as drowning, electrocution, burns and car accidents. Which training should a practitioner choose? Pat Ogden’s broader project of combining talk and body therapies into a cohesive psychotherapy model to work with trauma and attachment is the mainstay of the SP training in the way that Peter Levine’s broader project of utilizing the technique of discharging excess arousal as a means of trauma resolution is the mainstay of the SE training. Which training a student would find more helpful is a matter of individual choice based on professional training and interest. |
AuthorProsopon Therapy Archives
July 2024
Categories |
||||||
 RSS Feed
RSS Feed